Health is an essential contributor to an individual's lifespan. Human health and well-being are intimately linked to the state of the environment. The work environment constitutes a vital part of man’s total environment where he spends a considerable proportion of his daily life, so health, to a large extent, is affected by work conditions. Occupational environment plays a significant role in the health of those exposed to environmental pollutants. The health hazards get more severe when the duration of exposure increases. An occupational disease is a health condition or disorder caused by the work environment or activities related to the work.
Healthy workplace is one where employees and employers collaborate to improve workers' health, safety and well-being continuously. To a large extent, health is a function of workplace conditions. A workers spend a considerable hours of his day in the workplace.
The significant occupational diseases/ morbidity of concern in India are: silicosis, musculoskeletal injuries, coal workers’ pneumoconiosis, chronic obstructive lung diseases, asbestosis, byssinosis, pesticide poisoning and noise-induced hearing loss. The Directorate General of Factory Advisory Services and Labour Institutes (DGFASLI), Government of India, assists in formulation of national policies on occupational safety and health in factories and docks, and advises factories on the safety, health, efficiency, and well-being of workers.
As half the world’s population is living in urban settlements, millions in developing countries, suffer and die from respiratory diseases caused by air pollution. Effective workplace health and wellbeing programmes can positively impact worker productivity and performance and the health & well-being of employees, families and communities. The occupational environment plays a significant role in the health of those exposed to pollutants, and the health hazards get more severe when the duration of exposure increases. The occupational risk factors are responsible for about 13 percent of COPD, 11 percent of asthma, 9 percent of lung cancer and two percent of leukaemia that occur globally and constitute about 1.5 percent of the global burden of diseases in terms of Disability Adjusted Life Years (DALYs) (Xiaochen et al, 2020).
Workplace exposure to air pollution (particulate matter, gases and fumes) was responsible for 4,50,000 deaths/year (WHO, 2021). More than 12 million people around the world die every year because of unhealthy working environments. Occupational health was long ignored in India, and it was one of the components of the Sustainable Development Goals (SDGs), 2030 aimed “to ensure healthy lives and promote well-being” and “decent work” for all people (Healthy People-UN’s Agenda, 2030 Goal).
Need for the study:
The lungs are the only internal organs constantly exposed to the external atmosphere and are liable to get damaged when exposed to petrol/diesel fumes. According to the Global Burden of Disease report, air pollution is the fifth leading cause of death in India. India bears the most significant aspect of outdoor air pollution with one-fifth of global deaths occurring in India (Lelieveld et al, 2020). Personal protective equipment and other control measures can reduce respiratory problems.
Objectives
The study was set out with following objectives to: (1) assess the proportion of respiratory morbidity, and (2) associate the selected respiratory morbidities with selected demographic, occupational, past clinical and family health variables among employees of petrol filling stations in New Delhi; (3) assess the level of knowledge on lung health, level of pulmonary function parameters and level of respiratory morbidity; (4) evaluate the effectiveness of the pre-habilitation programme in terms of the level of knowledge on lung health, level of pulmonary function parameters and level of respiratory morbidity; (5) compare the effectiveness of the prehabilitation programme in terms of the level of knowledge on lung health, level of pulmonary function parameters and level of respiratory morbidity in post-tests; and (6) correlate the level of knowledge on lung health with pulmonary function parameters and respiratory morbidity among employees of petrol filling stations in the intervention and control groups in the post-test.
Review of Literature
A total of 86 studies, were organised under the following sections:
Section I: Overview of respiratory morbidity across the world and India (25)
Section II: Respiratory morbidity and its impact on employees of petrol filling stations (23)
Section III: Knowledge of respiratory morbidity and lung health among employees of petrol filling stations (14)
Section IV: Effectiveness of educational training programs on lung health among employees of petrol filling stations (24)
Methodology
Quantitative research approach was adopted for both Phase I and Phase II. For Phase, I, a descriptive survey design, and for Phase II quasiexperimental design (non-equivalent control group design) was adopted. The study was conducted at selected petrol filling stations, including the IGL Indraprastha CNG gas station under Bharat Petroleum Limited, Indian Oil Limited, and Hindustan Petroleum Limited in New Delhi.
According to the Annual Report (2021) prepared by the Delhi Traffic Police, there were over 1.22 crore registered vehicles of all categories. Delhi is covered with a decent number of petrol filling stations at regular intervals to meet the fuel needs of the increasing vehicular population. Many petrol filling stations and gas stations work around the clock. According to 2022 data of the Petroleum Planning and Analysis cell (Ministry of Petroleum and Natural Gas, there are 1273 petrol filling stations and 1400 IGL (Indraprastha Gas Limited) Compressed Natural Gas (CNG) stations in Delhi.
The sample for Phase I consists of all the available employees working in selected petrol filling stations in New Delhi; about 600 employees who fulfilled the inclusion criteria were included in the Phase I survey. Samples for Phase II consist of all employees working in selected petrol filling stations and who fulfilled the inclusion criteria. Sample size calculation: It was estimated using the comparison formula of population formula. The sample size was calculated based on the pilot study results.
To compensate for the attrition of 5 percent, the final sample size was rounded off to 200. Therefore, the total sample needed was 400 (200 samples for the intervention group and control group each). Sampling technique: Non-probability convenience sampling technique was used to select employees from selected petrol filling stations in New Delhi.
Description of the tool:The tool consists of four parts and sections as under.
Part 1: Socio-demographic proforma, Section A: Demographic proforma; Section B: Occupational variables;
Section C: Clinical health history and family health history.
Part 2: Physiological Parameters, Section A: Anthropometry and vital parameters; Section B: Pulmonary function parameters.Part 3: Structured questionnaire to assess the level of knowledge on lung health among employees of petrol filling stations.
Part 4: Questionnaire to assess the respiratory morbidity and risk factors (MRCQ - Medical Research Council, 1986, United Kingdom).
Intervention – Pre-habilitation Programme
Pre-habilitation is defined as improving a client's functional capability before any life-threatening conditions (American College of Surgeons, 2019). In the present study, the Prehabilitation Program consists of: Supportive education on knowledge of lung health, and Demonstration of breathing exercises. The breathing exercises include diaphragmatic or abdominal, pursed lip breathing, balloon blowing, and water bubbling exercises.
Data analysis:
The statistical tests, both descriptive and inferential statistics, were used to analyse the data collected in Phase I and Phase II.
Results
Table 1 depicts the distribution of cough and phlegm among employees of petrol filling stations. Half of the employees had a cough in the morning, and 51% expressed having a cough on a day or night. Nearly half (44%) of the employees had a cough with phlegm in the morning, and the same percentage had phlegm during the day or at night. And the same percentage (44%) of employees reported increased cough frequency with phlegm in the last three years. The majority, 93% of the employees, experienced at least one such episode of cough and phlegm in a year, and the remaining 7% had not experienced cough and phlegm episodes. Distribution of breathlessness and wheezing among employees of petrol filling stations. Regarding shortness of breath, 41% of employees had it while walking or climbing stairs. Among these, the majority (99.2%) of employees reported stopping or holding their breath for a while when walking. About 40% of employees had an attack of wheezing in the last year, and 38% of them had shortness of breath with wheezing. Among these (99.6%), employees had regular breathing episodes between attacks. About 38% of the employees had awakened during nighttime with an episode of shortness of breath in the last year, and the remaining 62% of them did not have shortness of breath. Table 2 illustrates that all employees (100%) in the intervention and control groups had an inadequate level of knowledge of lung health.
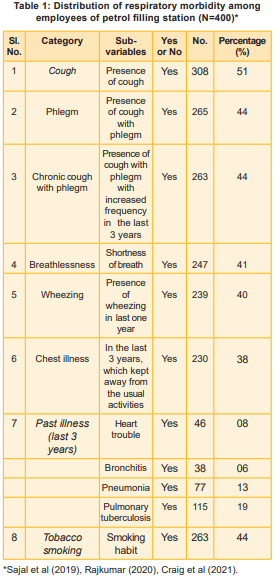
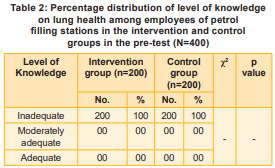
Table 3 exhibits the knowledge scores on lung health among employees in the intervention group between pre-test, post-test I and post-test II. The mean knowledge score in the pretest was 5.265, which improved after supportive education at the end of 4 weeks to 17.410 in post-test I (p<0.001). The knowledge score further improved at the end of 12 weeks to 20.085 in post-test II (p<0.001), which shows that the pre-habilitation was highly effective in improving he knowledge of the employees in petrol stations in the intervention group.
the intervention group between pre-test, post-test I and post-test II. The mean FVC value in the pretest was 2.134, which has increased to 2.822 in post-test I (p<0.001), and it further increased at the end of 12 weeks to 3.389 in posttest II, which was found to be significant (p<0.001) and reveals that the pre-habilitation programme was highly effective in improving the FVC value among employees of petrol filling stations. The mean FEV1 value in the pre-test was 2.642, which increased to 2.768 in post-test I (p<0.001). It increased at the end of 12 weeks to 3.446 in post-test II, which was highly significant (p<0.001) and reveals that the pre-habilitation programme was highly effective in improving the FEV1 value among employees of petrol filling stations. The mean FEV1/FVC ratio in the pre-test was 0.512, which has increased to 2.072 in post-test I (p<0.001), and it further increased at the end of 12 weeks to 2.960 in posttest II, which was found to be highly significant (p<0.001) and shows that the pre-habilitation programme was highly effective in improving the FEV1/FVC ratio among employees in the petrol filling stations. The mean PEFR value in the pretest was 297.100, which increased to 328.305 in posttest I (p<0.001), and it further increased at the end of 12 weeks to 361.875 in post-test II (p<0.001), which was found to be highly significant (p<0.001) and shows that the pre-habilitation programme
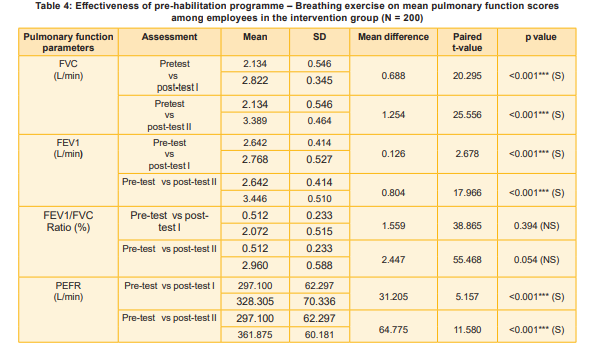
was highly effective in improving the PEFR value among employees of petrol filling stations.
Table 5 exhibits the mean difference in respiratory morbidity among employees in the intervention group between pre-test, post-test I and post-test II.
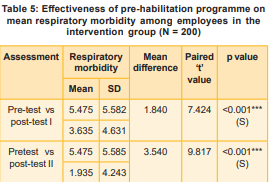
The overall mean respiratory morbidity score in the pretest was 5.475, reduced at the end of 4 weeks to 3.635 in post-test I (p<0.001). It further reduced at the end of 12 weeks to 1.935 in post-test II, which was found to be highly significant (p<0.001). The findings showed that the prehabilitation programme was highly effective in reducing respiratory morbidity among the employees of petrol filling stations.
Discussion
The present study showed the following respiratory morbidity data:
Occupational Variable
No association was found between Cough, Phlegm, Breathlessness and Wheezing Exposure to the type of pollutant - Risk factor (p<0.05).
Occupational category – Respiratory morbidity (p<0.05).
Conclusion
The work environment constitutes an essential part of man’s total environment, where he spends much of his daily life. Petrol pump workers are continuously exposed to the organic and inorganic substances in the petrol and diesel fumes, causing ill effects when exposed to higher concentrations and longer durations. The pre-habilitation programme consisted of supportive education and breathing exercise demonstrations, which created awareness, improved pulmonary function parameters, and helped overcome the employees' respiratory morbidities. The improvement in their variables is higher in post-test II than post-test I, which indicates longer practice yields better results. The pre-habilitation programme is highly effective, costeffective, time-saving, and feasible intervention, and this can be used by occupational health nurses in hospitals and industrial setups for the employees of petrol filling stations.
Nursing Implications
Nursing Service: Education on pre-habilitation programmes in the community and other family health set-up clinics should be carried out. Community health nurses should plan routine teaching on pulmonary function exercises for petrol filling station employees.
Nursing Education: The nurse educator can teach the students about pre-habilitation programmes, lung health education, and breathing exercises for vulnerable groups exposed to a polluted environment.
Nursing Administration: Rooms be provided for display of posters, videos, or demonstration sessions on the techniques of breathing exercises and booklets on the rehabilitation programmes in the OPD and wards.
Nursing Research: Studies can be conducted to assess the long-term effectiveness of prehabilitation programmes among the employees of petrol filling stations compared with the general population.
Recommendations
A similar study can be (1) replicated in large groups to generalise findings, (2) done among all employees in other high-risk occupational areas. Daily exercise will improve the lung health of the employees. Hence, cost-effective breathing exercises can be implemented in all petrol filling stations.
Conclusion
The pre-habilitation programme consisted of supportive education and breathing exercise demonstrations, created awareness, improved pulmonary function parameters and helped to overcome the respiratory morbidities of the petrol filling station employees. As it is a highly effective, time-saving and feasible occupational health measure, all occupational interventions can be conducted in all settings.
1. Alyami RM, Alhowikan AM, Alharbi AR, Al-Nafisah G. Impact of supervised exercise training on pulmonary function parameters, exercise capacity and irisin biomarker in interstitial lung disease patients. Pak J Med Sci 2020; 36 (5): 1089-95
2. Asia Abddelraoof, A.E., Fathima Rashid and Safa Kabashi, E.A. Knowledge of petrol station workers about the health effects from their occupation in Korari, Omdurman, Sudan. University of Science and Technology 2021; 21: 1-80
3. Wagh L, Laishram T, Jesse JM, Changsan JN, Kalane DS, Kamble AS. A descriptive study to assess the knowledge level on effects of inhaling vapours of petrol on health among petrol pump workers in selected areas of Pune City. International Journal of Applied Research 2021; 7(2): 206- 208
4. Labaki WW, Han MK. Chronic respiratory diseases: A global view. Lancet Respir Med 2022; 8(6): 531- 33
5. Mandal A, Mukherjee N. Pulmonary function of petrol filling workers from West Bengal, India. International Journal of Occupational Safety and Health 2020; 10(1): 28 -37
6. Kumar Manoj, Prashar Savita. A longitudinal study on respiratory morbidity due to air pollution in an industrial town Mandi Gobindgarh, Punjab, India. Medical Respiratory Case Study 2021; 6(s5): 25-29
7. Mohsin M, Yin H, Huang W, Zhang, Zhang L, Mehak A. Evaluation of occupational health risk management and performance in China: A case study of gas station workers. Intern J Environ Res Public Health 2022 March; 19(17): 3762-65
8. Muhsin F. Relation between working in petrol station and blood haemoglobin levels for the filling workers in Al-Najaf City, Iraq. Ind J Forensic Med & Toxicol 2020; 14(2): 565-69
9. Nkrumah ENK, Liu S, Doe Fiergbor D, Akoto LS. Improving the safety-performance nexus: A study on the moderating and mediating influence of work motivation in the casual link between Occupational Health and Safety Management (OHSM) practices and work performance in the oil and gas sector. Intern J Environ Res Public Health 2021 May; 8(5064): 1-23
10. Srivastava A, Barkule S. Airway function and mental health status of petrol pump workers of Aurangabad City, Maharashtra – An analytical cross-sectional study. J Clin Epidemiol Global Health 2020; 8: 661- 65
11. Xiochen Li, Abate D, Abate KH, James SL. Assessing global disability. Eur Resp Journal 2020; 53 (1): 31
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.