Palliative care is an essential component of comprehensive cancer management, addressing not only physical symptoms but also psychosocial, emotional, and spiritual needs of patients and their families. Nursing interventions begin with diagnosis and continue until the end of life, focusing on symptom relief, comfort, and quality of life. Palliative care is increasingly recognised as a global health priority due to the ageing population and rising burden of cancer and other non-communicable diseases. The World Health Organisation estimates that 56.8 million people worldwide require palliative care annually, with 25.7 million in their last year of life (WHO, 2014). However, over 87 percent of global opioid consumption is concentrated in high-income countries, leaving low- and middle-income nations including India with limited access to essential pain relief (INCB, 2020). India reports more than 1.1 million new cancer cases annually, with nearly 780,000 deaths. While advanced treatments extend survival, many patients live with distressing symptoms that adversely affect quality of life.
At Tata Memorial Hospital (TMH), the specialist palliative care OPD reported nearly 7,000 new registrations and over 36,000 consultations in 2021-2022 (NCRP, 2022), highlighting the increasing demand for outpatient palliative services that reduce hospital visits while ensuring timely support. Outpatient palliative care has been shown globally to improve symptom control, reduce unnecessary hospitalisations, and enhance patient satisfaction. Nurses, by virtue of their proximity to patients, are uniquely positioned to influence care quality and patient satisfaction (TMH Annual Report, 2022). Nursing interventions including medications, wound care, fluid management, and supportive counselling, play a central role in achieving these outcomes.
Despite this, there is limited Indian research systematically summarising nursing interventions and their outcomes in outpatient palliative care. Documentation of interventions, patient symptom relief, analgesic use, intravenous fluids, and wound care practices remains inconsistent, particularly with the growing adoption of electronic medical records (EMR). This gap underscores the need for systematic evaluation of nursing practices to inform evidence-based care, optimise patient outcomes, and strengthen the quality of palliative services in India.
Need for the study: Given the critical role of nurses in outpatient palliative care and the lack of comprehensive documentation studies in India, this study aimed to evaluate the number, types, and outcomes of nursing interventions at the TMH Palliative Care OPD to identify areas for documentation standardisation, EMR training, and integration of psychosocial care, ultimately enhancing patient safety and quality of care.
Operational Definition
Nursing intervention: Any procedure, treatment, or supportive care activity directly performed by a nurse and documented in the OPD record (eg, administration of IV fluids, wound dressing, pain management counselling).
Outcome measure: Documented change in patient status following a nursing intervention, recorded either during the same visit or at the next OPD follow-up.
Incomplete record: Missing information on the type of intervention, patient identifiers, or follow-up outcome.
Objectives
The study undertook to (i) evaluate the nursing interventions documented in the Specialist Palliative Care Outpatient Department (OPD) at TMH over six months, (ii) describe the number and types of nursing interventions recorded in the specialist Palliative Care OPD, and examine patient outcomes associated with these interventions, as documented either on the same day or during subsequent visits.
Methodology
This was a retrospective, exploratory descriptive study conducted to evaluate nursing interventions documented in the specialist Palliative Care OPD at Tata Memorial Hospital, Mumbai.
Study setting and period: TMH is a tertiary cancer centre where specialist palliative care services were initiated in 1996. The Palliative Care OPD operates Monday to Friday (9:00 am - 5:00 pm) and Saturday (9:00 am - 1:00 pm), with an average daily attendance of 100 to150 patients. Nursing documentation records of patients attending the OPD between 1 January 2023 and 30 June 2023 were reviewed. Data collection was conducted from 21 September 2023 to 18 October 2023.
Study population and sampling: The study population included adult patients who received nursing interventions in the Palliative Care OPD during the study period. A consecutive sampling method was employed, including all eligible patient records within the timeframe. Approximately 1000 patient records were initially screened; 903 records met the inclusion criteria, while 110 were excluded due to incomplete documentation. The final sample comprised 793 cases.
Eligibility criteria:
Inclusion criteria – Adult patients (≥18 years) registered in the Palliative Care OPD. Patients who had received at least one documented nursing intervention during the study period. Exclusion criteria – Incomplete or missing nursing documentation. Paediatric patients (<18 years). Adult patients referred but not registered in the OPD.
Tools for data collection: Data were extracted using a structured proforma developed by the investigators. Nursing interventions were identified from procedure books maintained in the palliative care OPD, Nursing documentation records integrated into patient case files, electronic medical records (EMR), where available
Nursing Interventions Assessed
Treatment and procedures: Specimen collection; administration of antibiotics, antipyretics, antiemetics, and analgesics; blood glucose testing; nebulisation; bleeding management; nasogastric tube insertion; intravenous fluids; Foley’s catheterisation; enema administration; wound dressing; tracheostomy care.
Supportive care: Pain management, nutritional support, and bed sore care.
Outcome Measures and Patient-Reported Outcomes
Patient outcomes were assessed based on documented improvement in symptoms or physical condition.
Pain: Reduction in self-reported pain intensity on a numerical rating scale (0-10).
Nausea/vomiting: Absence or reduction after administration of antiemetics, recorded as categorical responses (absent/mild/moderate/ severe).
Wound care: Documentation of reduced discharge, bleeding, or infection after dressing. Dyspnoea: Improvement in breathing pattern following nebulisation.
Documentation details:
Outcomes were primarily captured in structured fields within procedure books or EMRs to ensure consistency. Structured free-text entries were reviewed only to clarify interventions or outcomes when structured data were incomplete.
Ethical consideration:
The study was approved by the Institutional Ethics Committee. A consent waiver was obtained due to the retrospective nature of the study. All patient information was handled confidentially.
Data analysis:
Data were entered and analysed using SPSS version 25 (IBM Corp, Armonk, NY, USA). Exploratory data analysis was conducted to summarise the characteristics of the study population and nursing interventions. Descriptive statistics included frequency and percentage for categorical variables (eg, type of intervention, symptom improvement, gender, diagnosis). Mean and standard deviation for continuous variables (eg, patient age). For associations between interventions and symptom improvement, Chisquare tests were applied where appropriate.
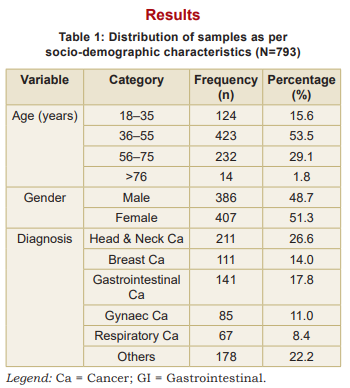
This study included 793 adult patients who attended the specialist palliative care OPD. The mean age of participants spanned a wide adult range, with the majority (53.5%) aged 36-55 years (Table 1). Patients aged 18-35 years accounted for 15.6 percent, those aged 56–75 years for 29.1 percent, and patients above 76 years constituted 1.8 percent of the cohort. Gender distribution was nearly balanced, with 407 females (51.3%) and 386 males (48.7%). Regarding diagnosis, the most common cancers were head and neck (26.6%), gastrointestinal (17.8%), and breast cancer (14.0%). Gynaecological cancers accounted for 11.0 percent, respiratory cancers for 8.4 percent, and other malignancies constituted 22.2 percent of cases.
It reflects the typical outpatient palliative population at a tertiary cancer centre, with a predominance of middle-aged adults and a wide variety of cancer types. The balanced gender distribution and diverse diagnoses underscore the heterogeneity of patient needs, highlighting the importance of individualised nursing interventions in symptom management.
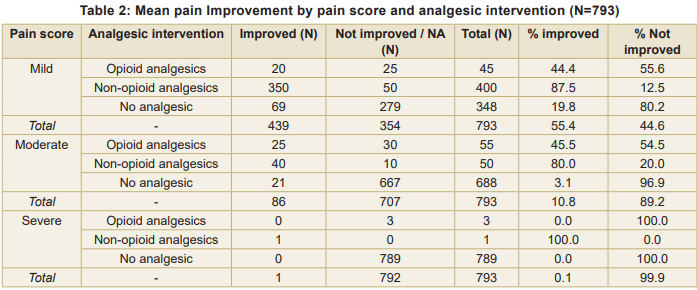
Mean pain improvement by pain score and analgesic intervention shows that in mild pain, non-opioid analgesics were most effective (87.5% improved), opioids moderately effective (44.4%), and improvement without analgesics was low (19.8%). Overall, 55.4 percent of patients improved. In moderate pain non-opioid analgesics led to 80 percent improvement, opioids 45.5 percent, and only 3.1 percent improved without analgesics. Overall improvement was 10.8 percent. In severe pain, most patients (789/793) received no analgesics and did not improve. A very small number received opioids (0% improved) or non-opioids (100% improved, n=1). Overall improvement was 0.1 percent. Chi-square analysis confirmed a highly significant association between type of analgesic intervention and pain improvement (χ² = 1,442.07, df = 2, p < 0.001). Non-opioid analgesics were highly effective in mild and moderate pain, while severe pain remains largely untreated, highlighting a critical gap in pain management (Table 2).
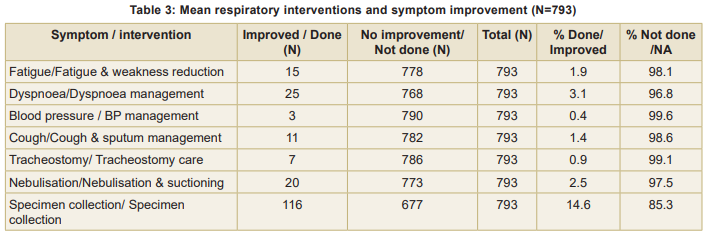
Table 3 shows that the most commonly performed intervention was specimen collection (14.6%), with a corresponding improvement in outcome. Other interventions, such as dyspnoea management and fatigue reduction, were less frequent (<5%) and showed minimal improvement in symptoms. Interventions like blood pressure management, tracheostomy care, and nebulisation were rarely performed (<3%). In the majority of patients no intervention was needed, hence no improvement.
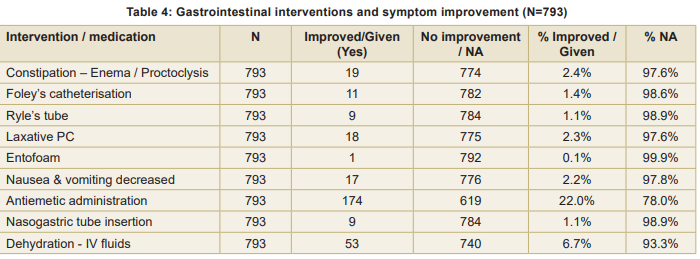
Mean gastrointestinal interventions and symptom improvement, the elimination needs and constipation management are shown in Table 4. Improvement rates were low for enema/proctoclysis (2.4%), Foley’s catheterisation (1.4%), Ryle’s tube (1.1%), Laxative PC (2.3%), and Entofoam (0.1%). Decrease in symptoms of nausea and vomiting was observed in 2.2 percent, whereas antiemetic administration was given in 22 percent of patients, reflecting preventive or therapeutic intervention. In dehydration management fluids led to symptom improvement in 6.7 percent of patients, and nasogastric tube insertion improved symptoms in 1.1 percent. Majority of patients (>90%) did not experience measurable short-term improvement in gastrointestinal symptoms.
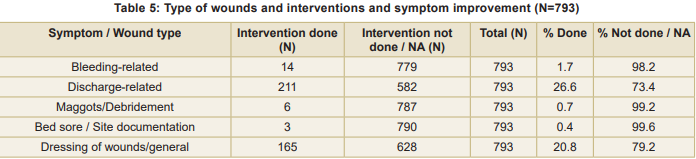
The distribution of wound-related interventions showed that certain wound types were more likely to receive nursing care than others (Table 5). Discharge-related wounds were the most commonly managed (26.6%), indicating a high prevalence and priority for intervention in the OPD setting. General wound dressings were documented in 20.8 percent patients highlighting the routine nature of dressing care as a nursing responsibility. Bleeding-related wounds were addressed in 1.7 percent cases reflecting either lower occurrence or selective intervention. Maggot-infested wounds (debridement) were rarely documented (0.7%), suggesting fewer cases or referral for specialised wound care. Bed sores - least frequent (0.4%), possibly due to in-patient management or preventive measures limiting their occurrence in OPD patients. Chi-square analysis showed a highly significant association between wound type and intervention (χ² = 573.47, p < 0.001). This indicates that common wound types (dischargerelated, general dressings) were substantially more likely to receive intervention compared to less frequent wound conditions (maggots, bleeding, bed sores).
Discussion
The most frequently documented symptoms were pain, fatigue, nausea, constipation, dyspnoea, ulcers, and dehydration. Our findings confirm
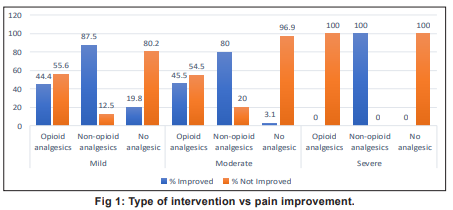
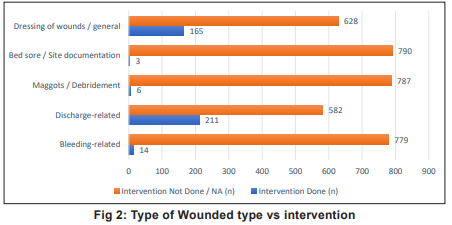
that timely and structured nursing interventions are pivotal in alleviating these common symptoms and improving patient comfort and quality of life. Pain management was the most frequently documented intervention, with effective relief observed in all cases receiving analgesics. This aligns with findings of Skjoedt et al who reported pain as the primary target of palliative nursing care although the proportion of pharmacological interventions was higher in our study (74%) compared to 42 percent in Western outpatient settings. Differences may reflect variations in patient demographics, cultural expectations, and accessibility of nursing resources in India. Bar charts of type of intervention vs pain improvement are depicted in Fig 1 and Fig 2.
Respiratory interventions, including dexamethasone administration and nebulisation, resulted in improvement in dyspnoea in 3.1 percent of patients. Gastrointestinal interventions, including antiemetics, intravenous fluids, and nasogastric tube insertions, were effective in a subset of patients, underscoring the importance of individualised symptom-focused care. Eliminationrelated interventions (proctoclysis/ enema, Foley catheterisation) and wound care (dressing, maggot removal) demonstrated the breadth of nursing responsibilities in the OPD highlighting the role of nurses in both procedural and supportive care.In Europe, the EAPC emphasises multidimensional symptom management addressing physical, psychological, social, and spiritual domains (EAPC, 2020). While our study confirms adherence to physical and pharmacological interventions, psychosocial and spiritual care were less frequently documented, indicating a gap in routine outpatient documentation practices in India. Similarly, Skjoedt et al. reported that pain and impaired physical function accounted for most interventions, whereas our study found wound care and pain management as the most frequent, reflecting resource availability, patient population needs, and cultural differences in symptom reporting.
Opioid access remains a known challenge in India due to regulatory and supply limitations, yet our study demonstrates that opioids were appropriately administered to 123 (15.5%) patients indicating progress towards aligning with international pain management standards.
A notable finding was the variation in documentation between nurses and physicians, with nursing records emphasising procedures, medications, and immediate patient-reported outcomes. Structured documentation, particularly using electronic medical records (EMR) could enhance continuity of care, quality assurance, and multidisciplinary communication (Campos et al, 2022; Singer et al, 2016). Training nurses in standardised EMR use may reduce documentation burden and facilitate inclusion of psychosocial and spiritual care domains, supporting holistic palliative care.
Strengths and Limitations
This study was among the first in India to comprehensively evaluate nursing interventions documented in a specialist palliative care OPD. The large sample size (N=793) enhances the reliability and generalisability of findings within tertiary care outpatient settings.
Key limitations include: Retrospective design relying on existing documentation, which may underreport psychosocial, spiritual, or unrecorded interventions; Exclusion of incomplete records, potentially introducing selection bias; Limited scope to measure long-term patient outcomes beyond the immediate follow-up visit.
Implications for Practice and Research
1. Standardisation of nursing documentation using structured EMR templates to capture both physical and psychosocial care components.
2. Training programmes for nurses on EMR use and holistic documentation practices to ensure comprehensive recording of interventions.
3. Incorporation of patient-reported outcomes in routine documentation to evaluate intervention effectiveness.
4. Future research using prospective designs to assess the impact of nursing interventions on quality of life, symptom control, and caregiver satisfaction.
Conclusion
Nursing interventions are integral to symptom management and supportive care in the palliative care outpatient setting. Pharmacological interventions remain the most frequently documented with wound care, fluid management, and other supportive measures contributing significantly to patient comfort. However, current documentation practices underrepresent psychosocial and holistic aspects of care.
Implementing standardised EMR-based documentation, including multidisciplinary notes can improve continuity and quality of care; support patient safety; and enable data-driven evaluation of nursing effectiveness. These measures reinforce the critical role of nursing in delivering comprehensive, patient-centred palliative care.
1. Finlay E, Casarett D, Smith T, Johnson R, Lee A, Kumar S, et al. Opioid use and symptom control in palliative care settings. J Palliat Med 2018; 21(4): 456-62
2. World Health Organization. Cancer pain relief. 2nd edn. Geneva: World Health Organization; 2019
3. International Narcotics Control Board. Availability of opioids: Global perspective. Vienna: United Nations; 2020
4. Singer PA, Bowman KW. Quality end-of-life care: A global perspective. Lancet 2016; 388(10054): 2024-35
5. Shore AD, Hicks RW, Morlock LL, Orav EJ, Keohane C, et al. Medication errors in palliative and end-of-life care. Arch Intern MedS 2010; 170(5): 421-29
6. Skjoedt T, Jensen AB, Ross L, Munk K, Groenvold M, Johnsen AT, et al. Advance care planning in patients with advanced cancer. Support Care Cancer 2019; 27(10): 3819-27
7. Shekhar S, Gupta R, Mehta R, Verma A, Singh P, Nair S, et al. Ethical challenges in palliative nursing practice. Indian J Palliat Care 2017; 23(3): 289-95
8. Parekh de CA, Levoy K, Pandey S, Wisniewski R, Brown J, Thomas M, et al. Global disparities in access to palliative care services. BMJ Support Palliat Care 2020; 10(2): e15
9. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: Palliative care. Version 2. Plymouth Meeting (PA): NCCN; 2022
10. World Health Organization. Palliative care [Internet]. Geneva: World Health Organization; 2020 [cited 2024 Jan 10]. Available from: https://www.who.int
11. Kumar S. Models of palliative care delivery in low- and middle-income countries. Indian J Palliat Care 2013; 19(2): 77-83
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.