Melioidosis is an infectious pathology instigated by the bacterium Burkholderia pseudomallei, which is commonly located in terrestrial and aquatic environments in Southeast Asia and northern Australia (Raja et al, 2005; Vidyalakshmi et al, 2007). The disease exhibits an extensive spectrum of clinical presentations, thereby complicating the diagnostic process (Jesudason et al, 2003). Presented below is a comprehensive case report that exemplifies the intricacies associated with melioidosis.
Need of the study:
Neurological melioidosis is a rare but severe manifestation of infection caused by Burkholderia pseudomallei, primarily found in tropical and subtropical regions (Viswaroop et al, 2007). While melioidosis commonly affects adults with underlying conditions like diabetes, its occurrence in previously healthy children is unusual and often misdiagnosed (Noyal et al, 2009). This case report highlights the need for increased clinical suspicion, early diagnosis, and timely intervention to prevent morbidity and mortality in paediatric patients. Documenting such rare presentations helps in guiding clinical practice and raising awareness, especially in endemic regions (Vidyalakshmi et al, 2007).
Review of Literature
Melioidosis, first described in 1911, is caused by the gram-negative bacterium Burkholderia pseudomallei (Raja et al, 2005). It is predominantly found in Southeast Asia and northern Australia but has also been reported in parts of India (Vidyalakshmi et al, 2007). Neurological involvement occurs in approximately 4 percent of all melioidosis cases, presenting as brain abscesses, encephalitis, meningitis, and cranial nerve palsies (Cheng et al, 2004). Children are less frequently affected than adults, and diagnosis is challenging due to its mimicry of conditions such as tuberculosis or viral encephalitis (Noyal et al, 2009). MRI and cultures are key diagnostic tools (Mukhopadhyay et al, 2007), and mortality rates are high if not treated early with appropriate antibiotics such as ceftazidime or meropenem (Sookpranee et al, 1992; Cheng et al, 2004).
Prevalence
Globally, melioidosis is endemic in Southeast Asia (Thailand, Malaysia, Singapore) and northern Australia (Raja et al, 2005). In these regions, protocols for early detection and treatment are better established (Cheng et al, 2004). Studies from Australia indicate a higher rate of central nervous system involvement in children, emphasising the pathogen’s neurotropic potential (Cheng et al, 2004). Climate change and increased travel have contributed to the emergence of melioidosis in nonendemic regions such as the Americas and parts of Africa (Vidyalakshmi et al, 2007).
Indian scenario:
In India, melioidosis is considered underreported due to limited diagnostic resources and lack of awareness (Vidyalakshmi et al, 2007). Southern and Eastern regions such as Tamil Nadu, Kerala, and Odisha have reported sporadic outbreaks (Mukhopadhyay et al, 2008). Pediatric neurological melioidosis is rarely documented, and many cases go misdiagnosed as tuberculous meningitis or cerebral malaria (Noyal et al, 2009). Awareness among paediatricians and inclusion of melioidosis in differential diagnosis in encephalitic illnesses is crucial, especially in endemic areas and post-monsoon periods (Cherian et al, 1996).
Epidemiology and risk factors:
B. pseudomallei is an environmental saprophyte endemic to Southeast Asia and northern Australia (Raja et al, 2005). It thrives in soil and water, primarily infecting individuals through direct contact, inhalation, or ingestion (Mukhopadhyay et al, 2008). While diabetes mellitus, chronic renal disease, and immunosuppression are well-known risk factors for severe melioidosis (Viswaroop et al, 2007), the index patient was previously healthy, emphasising the importance of maintaining a high degree of suspicion even in immunocompetent individuals from non-endemic areas (Noyal et al, 2009).
Clinical Manifestations and Diagnostic Challenges
Melioidosis exhibits a broad clinical spectrum, ranging from asymptomatic colonisation to severe sepsis and fulminant organ involvement (Jesudason et al, 2003). Neurological melioidosis, as seen in this case, is rare and often presents with encephalomyelitis, abscess formation, or brainstem dysfunction (Cheng et al, 2004). The diagnostic complexity was exacerbated by multiple negative cultures and non-specific imaging findings. Advanced microbiological techniques, such as PCR and MALDI-TOF mass spectrometry, may aid in early identification of B. pseudomallei (Mukhopadhyay et al, 2008).
Management and Treatment Considerations
Melioidosis requires a prolonged and staged treatment regimen to achieve successful outcomes. The intensive phase consists of intravenous antibiotics, typically ceftazidime, meropenem, or imipenem, followed by an eradication phase using oral trimethoprim-sulfamethoxazole to prevent relapse (Sookpranee et al, 1992; Cheng et al, 2004; Walsh et al, 1995). In severe or CNS cases,carbapenems such as imipenem or meropenem have demonstrated superior CNS penetration and efficacy (Cheng et al, 2004).
Case Report
A 10-year-old female child from Chennai, India, presented with fever, cough and both upper extremities paralysis initially, then lower extremities started paralysis. Two months prior, she was treated for fever with Ceftriaxone after a reactive Widal test. Despite initial treatment, her symptoms persisted and worsened over the past week, leading to his admission for further management.
Examination Findings
Overall appearance: The patient looked dehydrated, toxic, and feverish (102). Vital Signs: heart rate was 128 beats per minute, respiratory rate was 50 beats per minute, and blood pressure was 90/70 mm Hg.
Respiratory system: Bilateral crackles and bronchial breath sounds were detected on the left side.
Abdomen: Free no fluid, mild splenomegaly.
Musculoskeletal system: The right knee was swollen, and both ankles were erythematous and edematous.
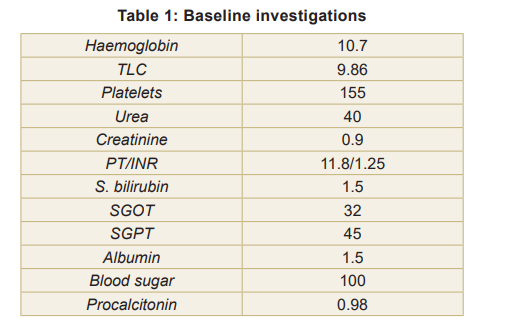
Laboratory Investigations (Table 1)
Haematological and biochemical parameters: Multiple parameters were deranged (specific values not provided).
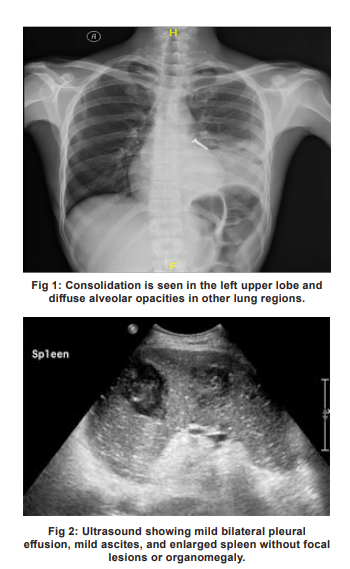
Imaging Results
Chest X-ray showed homogeneous consolidation in the left upper lobe and diffuse alveolar opacities in the remaining lung fields (Fig 1). The ultrasound revealed mild bilateral pleural effusion, mild ascites, and enlarged spleen without focal lesions or organomegaly (Fig 2). Brain biopsy results are depicted in Fig 3.
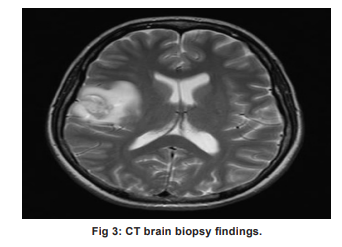
Brain biopsy results:
The biopsy of the parietal lesion indicated the presence of brain parenchyma with multiple abscesses, devoid of any mitotic tissue. Cultures yielded no growth. Following several episodes of generalised seizures, Levetiracetam was introduced, and the antitubercular therapy (ATT) was adjusted. After two weeks, the patient began to show signs of improvement; her fever decreased, seizures diminished, and she was able to walk with minimal assistance.
Clinical Course
After admission, the patient's condition worsened, leading to the development of acute respiratory distress syndrome (ARDS), with oxygen saturation levels plummeting to 78 percent. She was subsequently intubated and placed on mechanical ventilation. Empirical antibiotic treatment with Piperacillin/Tazobactam and Clindamycin was commenced.
Microbiological findings: Blood cultures identified Burkholderia pseudomallei, confirming a diagnosis of melioidosis. The organism demonstrated sensitivity to Imipenem.
Treatment and Outcome
The antibiotic regimen was modified to include Imipenem. Over time, the patient exhibited clinical improvement and was successfully weaned off the ventilator. She completed the intensive phase of antibiotic treatment and was discharged with a plan for extended eradication therapy.
Nurses’ responsibilities:
Nurses play a pivotal role in the management of children with neurological melioidosis. Their responsibilities include:
Early recognition and reporting: Identifying unusual symptoms (e.g., seizures, altered sensorium) and promptly reporting to physicians.
Infection control: Implementing standard precautions to prevent nosocomial infections, especially in ICU settings.
Medication administration: Ensuring timely and correct administration of intravenous antibiotics like ceftazidime, meropenem.
Monitoring and supportive care: Frequent neurological assessments, monitoring for signs of raised intracranial pressure, and managing fever, seizures, or altered consciousness.
Family education and support: Explaining the disease process, treatment plan, and prognosis to caregivers in a compassionate manner.
Documentation: Accurate recording of clinical observations, interventions, and responses to therapy for medico-legal and continuity-of-care purposes.
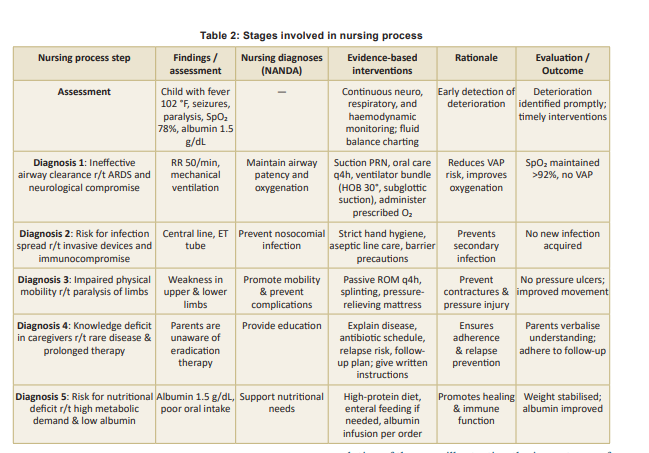
Stages of nursing process are outlined in Table 2.
Learning Points:
This case underscores several critical aspects of neurological melioidosis:
1. Diagnostic vigilance – Melioidosis should be considered in patients with neurological symptoms and unexplained infectious syndromes, especially in endemic regions. Negative cultures do not rule out the disease, and additional diagnostic modalities should be pursued.
2. Multisystem involvement – The presentation of pulmonary, musculoskeletal, and neurological symptoms suggests disseminated infection, requiring comprehensive evaluation and management.
3. Early antimicrobial optimisation – The use of carbapenems in severe cases significantly improves outcomes, and treatment must be prolonged to prevent relapse.
4. Severe disease potential – The risk of ARDS and multi-organ dysfunction necessitates intensive monitoring and aggressive supportive care in critically ill patients.
Despite the delayed diagnosis and severe disease course, the patient survived due to the timely escalation of therapy, illustrating the importance of recognising and managing neurological melioidosis effectively. Future advancements in rapid diagnostic testing may help in earlier detection and better clinical outcomes.
Conclusion
This case emphasises the need to document the occurrence of melioidosis in India. The diagnosis was likely overlooked due to insufficient clinical awareness and inadequate microbiological identification. A high level of suspicion is essential for diagnosis, given the varied clinical presentations. Additionally, this case underscores the necessity for enhanced microbiology services in patient care management. Successful treatment was achieved through the administration of appropriate antimicrobials based on the identified pathogen.
1. Raja NS, Ahmed MZ, Singh NN. Melioidosis: An emerging infectious disease. Journal of Postgraduate Medicine 2005; 51 (2): 140-45
2. Vidyalakshmi K, Shrikala B, Bharathi B, Suchitra U. Melioidosis: An underdiagnosed entity in western coastal India: A clinico-microbiological analysis. Indian Journal of Medical Microbiology 2007; 25 (3): 245-48. https://doi. org/10.4103/0255-0857.34767
3. Anuradha K, Meena AK, Lakshmi V. Isolation of Burkholderia pseudomallei from a case of septicaemia: A case report. Indian Journal of Medical Microbiology 2003; 21(2): 129-32
4. Jesudason MV, Anbarasu A, John TJ. Septicaemic melioidosis in a tertiary care hospital in South India. Indian Journal of Medical Research 2003; 117: 119-21
5. Viswaroop BS, Balaji V, Mathai E, Kekre NS. Melioidosis presenting as genitourinary infection in two men with diabetes. Journal of Postgraduate Medicine 2007; 53(2): 108-10. https://doi.org/10.4103/0022-3859.32210
6. Noyal MJ, Harish BN, Bhat V, Parija SC. Neonatal melioidosis: A case report from India. Indian Journal of Medical Microbiology 2009; 27(3): 260-63. https://doi. org/10.4103/0255-0857.53213
7. Sudhakar M, Dhakshinamoorthy S, Gnanarani J Satchi NS. Effectiveness of web quest on high alert medications upon knowledge among nursing students, Chennai. Research Journal of Pharmacology & Pharmacodynamics 2023; 15(3): 99-102 https://doi.org/10.52711/2321- 5836.2023.00018
8. Cherian T, John TJ, Ramakrishna B, Lalitha MK, Raghupathy P. Disseminated melioidosis. Indian Pediatrics 1996; 33 (5): 403-06
9. Balaji V, Rajiv K, Abraham OC. Burkholderia pseudomallei recovered in an HIV-positive individual. Indian Journal of Medical Sciences 2008; 62(11): 456-58
10. Sudhakar M, Dhakshinamoorthy S. Awareness regarding antibiotic stewardship among nurses at selected hospitals, Chennai. Research Journal of Pharmacology & Pharmacodynamics 2021; 13 (3): 86-88. https://doi. org/10.52711/2321-5836.2021.00018
11. Mukhopadhya A, Balaji V, Jesudason MV, Amte A, Jeyamani R, Kurian G. Isolated liver abscess in melioidosis. Indian Journal of Medical Microbiology 2007; 25 (2): 150- 51. https://doi.org/10.4103/0255-0857.32724
12. Dhodapkar R, Sujatha S, Sivasangeetha K, Prasanth G, Parija SC. Burkholderia pseudomallei infection in a patient with diabetes presenting with multiple splenic abscesses and abscess in the foot: A case report. Cases Journal 2008;1(1): 224 https://doi.org/10.1186/1757-1626-1-224
13. Mukhopadhyay C, Chawla K, Krishna S, Nagalakshmi N, Rao SP, Bairy I. Emergence of Burkholderia pseudomallei and pandrug-resistant non-fermenters from southern Karnataka, India. Transactions of the Royal Society of Tropical Medicine & Hygiene 2008; 102 (Supplement 1): S12-S17. https://doi.org/10.1016/S0035-9203(08)70005-1
14. Sookpranee M, Boonma P, Susaengrat W, Bhuripanyo K, Punyagupta S. Multicenter prospective randomized trial comparing ceftazidime plus co-trimoxazole with chloramphenicol plus doxycycline and co-trimoxazole for treatment of severe melioidosis. Antimicrobial Agents and Chemotherapy 1992; 36 (1) 158-62. https://doi.org/10.1128/ aac.36.1.158
15. Walsh AL, Smith MD, Wuthiekanun V, White NJ. Postantibiotic effects and Burkholderia (Pseudomonas) pseudomallei: Evaluation of current treatment. Antimicrobial Agents and Chemotherapy 1995; 39(10): 2356-58. https:// doi.org/10.1128/aac.39.10.2356
16. Cheng AC, Fisher DA, Anstey NM, Stephens DP, Jacups SP, Currie BJ. Outcomes of patients with melioidosis treated with meropenem. Antimicrobial Agents and Chemotherapy 2004; 48(5): 1763-65. https://doi.org/10.1128/ AAC.48.5.1763-1765.2004
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.