Astroke is a medical condition in which poor blood flow to the brain causes cell death. It is the rapid loss of brain functions due to a carotid artery block in the blood supply system (WHO, 2022). Studies conducted to examine the recovery of hemiplegic stroke patients show that up to 85 percent of patients have an initial deficit in the arm. While recovery of arm function is a poor in many patients, leg function has proven to be less of a problem. For upper limb rehabilitation, many therapeutic approaches are available. Recent studies have shown that motor imagery (MI) training can reduce arm impairment and activity limitations in people living with the effects of stroke; MI has had some degree of successful outcome in the acute, sub-acute and chronic populations of adults with stroke (Mulder, 2007).
One of the prospective randomised controlled trials recruited 42 subjects with chronic stroke. The intervention group received instruction regarding the Graded Motor Imagery (GMI) training and performed it at home over 8 weeks (30 minutes a day). The primary outcome measure was the change in motor function between baseline and eight weeks, assessed by the Manual Function Test (MFT) and Fugl Meyer Assessment (FMA). The secondary outcome measure was the change in the Activity of Daily Living (ADL), assessed with the Modified Index (MBI). Results showed that 37 of the 42 subjects completed the 8-week programme (17 in the GMI group and 20 controls). All subjects showed significant improvements in the MFT, FMA and MBI over time (p<.05). However, the improvements in the total scores for the MFT, FMA and MBI did not differ between the GMI and control groups. The MFT arm motion score for the GMI and control group was significantly better than that of the controls (p<0.05). They concluded that the motor imagery programme was useful for improving upper limb function as an adjunct to conventional rehabilitation for patients with chronic stroke (Ji et al, 2021).
Upper limb motor deficits were the most common problem among stroke survivors and most of the stroke survivors were unable to carry out the activities of daily living independently. To tackle the situation, it was felt that motor imagery training could effectively improve upper limb functions among patients with stroke.
Review of Literature
A prospective community-based study of stroke was conducted in Kolkata to determine the subtypes, prevalence, incidence, and case fatality rates of stroke. This longitudinal descriptive study comprised a two-stage, door-to-door survey of 52,377 individuals selected through stratified random sampling. The study showed that the overall case fatality rate was among the highest categories of stroke fatality in the world, with women having higher incidence and case fatality rates compared with men (Das et al, 2010).
A study assessed whether motor imagery might improve upper limb strength through an ecological approach and validation, using complex and multi-point exercises. Nine participants were included in the motor imagery group and 10 in the control group. The two-groups performed identical bench press and leg press exercises. The MI group was instructed to visualise and feel the corresponding contractions during the rest period, whereas the control group did a neutral task. The maximal voluntary contraction (MVC) and the maximal number of repetitions (MR) using 80 percent of the pre-test MVC weight were measured. Although both the MI and control groups enhanced their strength through the training, the leg press MVC was significantly higher in the MI group than in the control group (p<0.05) (Carrasco & Cantalapiedra, 2016).
Objectives
1. Test the effect of motor imagery training on upper limb function among patients with stroke.
2. Find the association between upper limb function among patients with stroke and selected variables among patients with stroke.
Hypothesis
H1- There is a significant difference between the mean improvement in the upper limb function score of the experimental and control group at the 0.05 level of significance.
H2- There is a significant difference between the mean reduction in the time taken for the tasks performed by the experimental and control group at the 0.05 level of significance.
H3- There is a significant association between upper limb function and selected patient variables at the 0.05 level of significance.
Materials and Methods
The research approach was quantitative and experimental, with two groups of pre-test and posttest design to assess the effect of motor imagery training on upper limb function among stroke patients.
Inclusion criteria: All patients, diagnosed with stroke with upper limb weakness, willing to participate in the study, knowing English or Malayalam, and with upper limb dysfunction were included.
Exclusion criteria: Patients having severe cognitive impairments, those with musculoskeletal problems, sensory aphasia, or hearing impairment and peripheral neuropathy were excluded.
Setting of the study: The study was conducted in the stroke rehabilitation units of Baby Memorial Hospital and Nirmala Hospital, Kozhikode (Kerala).
Sample size was calculated based on a previous study by Magdalena Ietswaart on motor imagery in stroke recovery (n=59.8 ≈ 60). However, due to feasibility, 40 participants were recruited, 20 each in the experimental and control group admitted to neurology wards and ICUs. Participants were selected using simple random sampling through a computer-generated allocation (A, C=experimental; B, D=control).
Data Collection Tools
(1) Personal and clinical data sheet; (2) Wolf Motor Function Test (WMFT) - a validated tool assessing upper limb strength, quality of movement, and task completion time; and (3) Motor activity record for documenting practice adherence.
Data collection procedure:Ethical approval was obtained from the concerned authorities of both hospitals. Informed consent was taken from patients and their relatives. Data was collected between 27 March 2023, and 22 April 2023. Pretest assessments were conducted for both groups using WMFT.
The experimental group received motor imagery training for 20 minutes daily, starting from day 2 of admission and continued at home for two weeks post-discharge, guided by audio instructions. Participants maintained activity records and were contacted regularly by phone. The control group received only conventional therapy. Post-test assessments were done for both groups at the end of the third week. After the post-test, the control group was also provided with instructions and audio material for motor imagery training. Collected data were coded and analysed using descriptive and inferential statistics. Mean, standard deviation, frequency, and percentage were used for descriptive statistics. Independent t-test and paired t-test were applied to determine the effectiveness of the intervention, Chi-square test/ANOVA was used to find associations with selected variables significance level p < 0.05).
Results
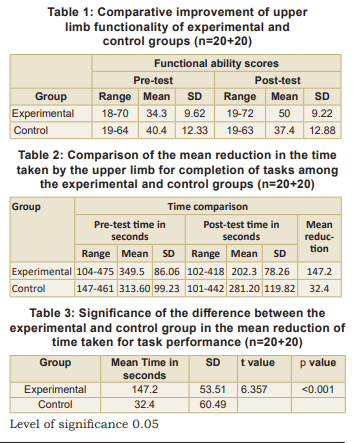
The subjects were distributed across various age groups, with the majority in both the groups between 51-60 years. Only 10 percent of subjects in the experimental group were below 50 years. Out of 40 participants, 55 percent in the experimental group and 65 percent in the control group were males. (Results in Tables 1-5).
Most subjects in both groups had a middle cerebral artery stroke, while the rest had posterior cerebellar artery involvement. The majority of participants in both groups had school-level education, and most were unemployed (65% in the experimental group and 50% in the control group). In both groups, the majority had ischaemic stroke (80% in the experimental group and 75% in the control group). Most subjects had comorbidities such as hypertension, diabetes mellitus, and dyslipidaemia. About 65 percent in both groups had diabetes; 55 percent in the experimental group and 75 percent in the control group had hypertension.
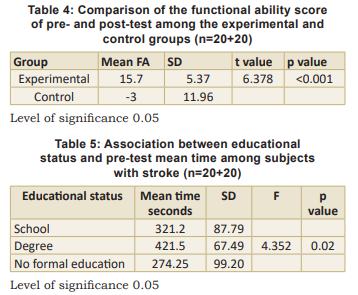
The effect of motor imagery training was assessed using WMFT. In the experimental group, the mean time for task completion reduced from 349.5 seconds (pre-test) to 202.3 seconds (post-test). Independent t-test analysis showed a significant reduction in time in the experimental group compared to the control group. Functional ability scores (mild, moderate, severe) also showed significant improvement in the experimental group after the intervention. Hence, motor imagery training was found highly effective in improving upper limb function among stroke patients. Analysis revealed a significant association between educational status and pre-test mean time taken to complete WMFT tasks.
Discussion
Our study found that the majority of the subjects (65%) were in the age group 50–60 years, and most were males (65%). The age-wise distribution indicated that stroke incidence was highest between 50-60 years, whereas only a few subjects (10%) were below 50 years of age. The study also revealed that the majority of patients in both the experimental (80%) and control (75%) groups had schematic stroke. Similar findings have been reported by Sridharan et al (2009).
Similar retrospective cohort study was conducted in a single centre stroke clinic in Navi Mumbai with the age groups 15-30 years, 31-45 years, 46-65 years and above 65 years. After the statistical analysis, a total of 1377 patients of acute stroke were identified, of which 12466 were ischaemic stroke, and 131 were haemorrhagic strokes. In this study, the mean age was 49.06 years, and 53 percent of males were affected. Their findings (Ekker et al, 2019; Kalita et al, 2023) were very similar to ours.
In our study, the functional ability scores of the experimental group, assessed using the WMFT, improved from a mean of 41.1 (pre-test) to 48.25 (post-test), indicating a significant improvement after motor imagery training. These findings show that motor imagery training effectively enhanced upper limb functional performance among stroke patients. Similar results were observed in a study that assessed whether motor imagery could improve upper limb strength through an ecological approach. Participants in the motor imagery group were instructed to visualise and feel the corresponding contractions during rest periods, while the control group performed a neutral task. Although improvement was noted in both groups, the motor imagery group showed significantly greater enhancement in strength compared to the control group, supporting the effectiveness of motor imagery in rehabilitation (Hatem et al, 2016; Wolf et al, 2005).
Another similar study was conducted in SVNIRTAR, Odisha (India) with 15 subjects in each group. The control group received conventional occupational therapy only, while the experimental group received conventional therapy combined with a motor imagery programme. The experimental group showed significant improvement compared to the control group (p < 0.004 and p < 0.001).
In the present study, a post-test was conducted two weeks post-intervention. The pre-test mean functional ability score of the experimental group was 40.4, which improved to 50.0 in the post-test. The difference was tested using a paired sample t-test, and the calculated t-value was 13.186 with a p-value of <0.001, confirming that motor imagery training was effective. Hence, it was concluded that there was a significant improvement in both time taken and functional ability scores of the experimental group who performed motor imagery training (Thankamani, 2015).
Nursing Implications
Nursing practice: Motor imagery training improves upper limb function in stroke patients, prevents disuse, and promotes early independence in daily living. The training protocol developed can serve as a resource for health professionals and caregivers, and as reference material for home-based care.
Nursing administration: Nurse administrators can promote awareness and integration of motor imagery training into stroke care, collaborate with healthcare bodies to adopt evidence-based practices to improve patient outcomes.
Nursing education: Nurse educators must update their knowledge on complementary therapies and foster research-based practice. Students should be encouraged to engage with stroke patients.
Nursing research: Administrators and managers should support studies exploring its benefits and use findings to guide future action plans.
Limitations: Small sample size (40 patients) limits generalisation. Grip strength assessment was difficult due to the lack of a dynamometer. Followup through telephone and post-test participation was inconsistent.
Recommendations: Replicate the study with larger samples in varied settings; Assess long-term effects of motor imagery therapy; Conduct periodic followup studies and comparative studies with other rehabilitative techniques; Explore centre-based motor imagery programmes; Conduct qualitative studies on the lived experiences of stroke patients receiving motor imagery.
Conclusion
Motor imagery training is effective in improving upper limb motor functions and can be incorporated into stroke rehabilitation. Nurses can play a crucial role in training patients to perform motor imagery, and this practice can also be effectively carried out at home under the guidance of a caregiver. Patients with mild functional deficits can perform the activity independently. The study also revealed a significant difference when outcomes were compared with selected variables.
1. World Health Organization. WHO EMRO | Stroke, Cerebrovascular accident | Health topics. WHO 2022. https://www. emro.who.int/healthtopics/strokecerebrovascularaccident/ index.htm
2. Mulder Th. Motor imagery and action observation: cognitive tools for rehabilitation. Journal of Neural Transmission 2007 Oct 1; 114 (10): 1265-78. https://www.ncbi.nlm.nih.gov/ pmc/articles/PMC2797860/
3. Ji EK, Wang HH, Jung SJ, Lee KB, Kim JS, Jo L, et al. Graded motor imagery training as a home exercise program for upper limb motor function in patients with chronic stroke. Medicine 2021 Jan 22; 100(3): e24351
4. Das SK, Banerjee TK, Biswas A, Roy T, Raut DK, Mukherjee CS, et al. A prospective community-based study of stroke in Kolkata, India. Stroke 2010 Dec; 41 (12): 2965-68. https:// www.ahajournals.org/doi/abs/10.1161/
5. García Carrasco D, Aboitiz Cantalapiedra J. Effectiveness of motor imagery or mental practice in functional recovery after stroke: A systematic review. Neurología 2016 Jan; 31 (1): 43–52. https://www.sciencedirect.com/science/article/ pii/
6. Ekker MS, Verhoeven JI, Vaartjes I, van Nieuwenhuizen KM, Klijn CJM, de Leeuw FE. Stroke incidence in young adults according to age, subtype, sex, and time trends. Neurology 2019 Apr 24; 92(21): e2444–54
7. Hatem SM, Saussez Geoffroy, della Faille M, Prist Vincent, Zhang Xue, Dispa Delphine, et al. Rehabilitation of motor function after stroke: A multiple systematic review focused on techniques to stimulate upper limb recovery. Front Hum Neuroscience 2016 Sep 13; 10-2016. https//doi. org/10.3389/fnhum.2016.00442
8. Thankamani Rajesh T. Effects of motor imagery on upper limb functional task performance and quality of life among stroke survivors. Disability, CBR & Inclusive Development 2015 May
9; 26(1): 109. DOI:10.5463 /DCID.V26i1.225 9. Kalita J, Bharadwaz MP, Aditi A. Prevalence, contributing factors, and economic implications of strokes among older adults: A study of North-East India. Scientific Reports 2023 Oct 6 13(1): 16880. https://www.nature.com/articles/ s41598-023-43977-z
10. Wolf SL, Thompson PA, Morris DM, Rose DK, Winstein CJ, Taub E, et al. The EXCITE Trial: Attributes of the Wolf Motor Function test in patients with subacute stroke. Neurorehabilitation and Neural Repair 2005 Sep; 19(3): 194-205
11. Sridharan SE, Unnikrishnan JP, Sukumaran S, Sylaja PN, Nayak SD, Sarma PS, et al. Incidence, types, risk factors, and outcome of stroke in a developing country. Stroke 2009 Apr; 40 (4): 1212-18
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.