Adolescence is a critical period of physical, psychological, and social change, during which antisocial behaviour (ASB) - persistent aggression, non-compliance, violence, and norm violation - can emerge as a major public health concern (Loeber & Farrington, 2012). Frequent ASB predicts adverse adult outcomes, while occasional rebellion may reflect normal development (Loeber et al, 2009; Odgers et al, 2008). ASB risk is shaped by family environment, peer influence, socioeconomic stressors, and exposure to violence, with early exposure and onset before age 15, predicting long-term behavioural disorders (Moffitt, 1993; Fergusson et al, 2008). In India, rapid urbanisation, peer pressure, and limited psychosocial support have intensified adolescent ASB, contributing to aggression, substance abuse, and crime (Lahey & Waldman, 2005). Studies from Northeast India report high prevalence of aggression and substance use, linked to lifestyle factors such as poor sleep and drug use (Espinoza-Romero et al, 2022; UNHabitat, 2013; Ningombam et al, 2022). However, adolescents’ knowledge and practices regarding ASB in this region remain poorly studied. Limited awareness and inappropriate practices may sustain ASB and weaken interventions. This study therefore assesses ASB-related knowledge and practices among 15-19-year-old students in a school in Imphal and examines their associations with demographic factors and with each other.
Objectives
The study was conducted with following objectives:
- To measure the amount of knowledge and the behaviours associated with antisocial activities among 15-19 years old students who are in one of the schools in Imphal (Manipur);
- To find out the demographic variables linked with knowledge and practices, and to look into the connection between knowledge and practices surrounding ASB; and
- To guide nurses, educators, and policymakers in developing targetted preventive and educational strategies so as to reduce ASB and promote safer school environments.
Methods & Materials
To evaluate the comprehension and habits about ASB among youth, a descriptive research design with a quantitative approach was used. This design was believed suitable to outline the current condition of the phenomena without altering any variables. Study setting and population: The location of the study was Lamlong Higher Secondary School, Imphal East (Manipur), which is the largest government school in the area. The target population consisted of the students that met the eligibility requirements.
Eligibility criteria: The students aged 15-19 years who were enrolled at the selected school, present throughout the period of data collection, students who were willing to participate, able to understand English, and capable of providing the required information, were included. For students aged 15-17 years, informed written consent (IWC) was obtained from the participants and also from their parents or guardians; students aged 18-19 years provided IWC independently. This IWC process ensured ethical compliance and protection of participants’ rights. Students below 15 years or above 19 years of age, those unwilling to participate, those unable to understand English, students who were absent throughout data collection, and those who participated inside the pilot study were left out from the study.
Sample size (SS) and sampling technique: Based on ubiquity estimates from previous studies and power analysis, an SS of 100 students was determined to be adequate. Participants were selected utilising a non-probability purposive sampling technique, ensuring inclusion of students as per the eligibility criteria. The SS for the present work was determined per findings from a previous similar study assessing knowledge and practices related to antisocial behaviour among adolescents. Assuming a prevalence of inadequate knowledge of 50 percent, a 95 percent confidence level, and a permissible error of 10 percent, the SS was calculated utilising the standard formula for single-population proportion:
n = Z²pq / d², where Z = 1.96 at 95 percent confidence, p = estimated prevalence, q = 1 − p, and d = allowable error. The calculated minimum SS was 96, which was rounded to 100, to account for possible non-response and to ensure adequate statistical power.
Power analysis was conducted to determine an adequate SS for the study, with reference to a previous study on antisocial behaviour among school-going adolescents reported by Singh et al (2019). The SS was calculated utilising the standard formula for estimating a single population proportion: n = Z²pq / d², where n is the required SS, Z is the standard normal deviate at 95 percent confidence level (1.96), p is the estimated prevalence of inadequate knowledge (assumed as 50% based on the referenced study), q = 1 − p, and d is the allowable error (10%). The calculated SS was 96, which was rounded to 100 to enhance statistical power and account for possible non-response, thereby ensuring adequate precision and reliability of study findings.
Data Collection Tools
Data was obtained utilising a self-developed structured questionnaire, which consisted of three sections (A, B and C).
Section A: Seven demographic variables (age, gender, educational status, family type, religion, family history of antisocial behaviours, dietary pattern) assessing the student’s information.
Section B: Thirty items assessing knowledge of antisocial behaviour, covering introduction, causes, impacts, and prevention management. Each correct response was then awarded one point, with knowledge levels categorised as poor (≤50%), average (51-75%), and adequate (>75%).
Section C: It had 19 items assessing practices related to antisocial behaviour utilising a checklist of negative behaviours with yes (0 point) or no (1 point) responses. Practices were categorised as bad (≤50%) and good (>50%).
Validity and reliability of tools: The instrument was validated by a panel of seven experts, including psychiatrists and nursing faculty. Reliability was tested utilising the Guttman Split-Half Coefficient method on a pilot sample of 10 students, yielding a coefficient of 0.772, which confirms acceptable reliability.
Content validity: Validity of the self-structured knowledge and practice questionnaire on antisocial behaviour was established utilising the Content Validity Index (CVI) method. The tool was reviewed by a panel of seven experts comprising psychiatrists and nursing faculty, who gauged each item for relevance, clarity, and adequacy utilising a four-point rating scale. Item-level Content Validity Index (I-CVI) and Scale-level Content Validity Index (S-CVI/Ave) were calculated. The overall S-CVI/Ave of the tool was found to be acceptable (>0.80), indicating good content validity. Necessary modifications were made to the questionnaire based on expert suggestions before final data collection.
Data Collection Procedure
Data acquirement was done for over one month (31 July to 29 August 2023). After obtaining institutional and school-level permission, IWC was secured from participants. Its purpose was explained, and anonymity alongside confidentiality were assured. The questionnaires were administered in classroom settings with approximately 20 students per session. Each participant was scheduled from 10:00 am upto 12:00 pm to complete the tool. Ethical considerations: Ethical approval was solicited from the Institutional Ethical Committee of the College of Nursing, Kangleipak Medical and Nursing Institute, Imphal. IWC permission was then also secured from school authorities. IWC was received from all participants, and data confidentiality was upheld throughout the study.
Data Analysis
Data was coded and then analysed utilising the Statistical Package for Social Sciences (SPSS) version 20. Descriptive statistics (frequency, percentage, mean, standard deviation) were utilised to summarise demographic characteristics and levels of knowledge and practices. Inferential statistics, counting chi-square tests alongside Pearson’s correlation, were applied to examine associations across knowledge and practices and selected demographic variables, and to determine correlations between knowledge and practices.
Results
Demographic characteristics of participants:
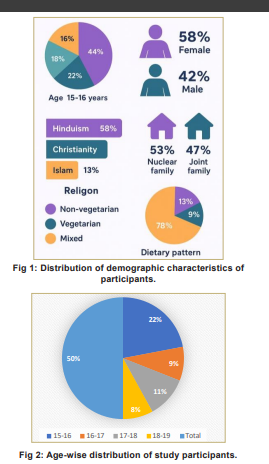
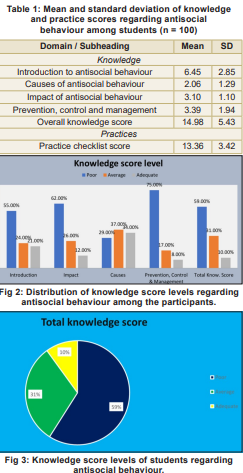
One hundred students aged 15-19 years participated in the study. Fig 1 presents the distribution of demographic variables. Most participants (44%) were aged 15-16 years, followed by 17-18 years (22%), 16-17 years (18%), and 18-19 years (16%). Females constituted 58 percent of the sample, while 42 percent were males. A total of 53 percent students were from Class XII, while the rest were from Class XI (5%) and Class X (42%). With respect to family type, 53 percent of the students belonged to nuclear families, whereas 47 percent were from joint families. Hinduism was the predominant religion (58%), followed by Christianity (25%) and Islam (13%). A family history of antisocial behaviour was reported by 30 percent of respondents. Regarding dietary pattern, 13 percent were non-vegetarians, 9 percent were vegetarians, and the remaining were mixed (78%).
Knowledge of antisocial behaviour:
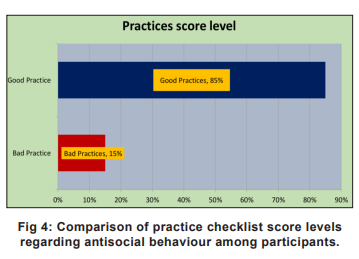
The knowledge score levels of students regarding antisocial behaviour are shown in Fig 2. The column chart illustrates the levels of knowledge in terms of introduction, impact, causes, prevention, control, and management. Findings from Figure 3 reveal that 59 percent of the students have poor knowledge (≤50%), 31 percent possess average knowledge (51-75%), and only 10 percent have adequate knowledge (>75%). These results indicate that nearly half of the participants lack essential understanding of antisocial behaviour, its causes, and its prevention. The overall mean score for students aged 15 to 19 years from a selected school regarding antisocial behaviour (Table 1) is 14.98±5.433, with an average knowledge distribution of 49.7 percent across the questions. Among the students, 6.45±2.851 know the area of introduction to antisocial behaviour, and an average of 53.8 percent understand this area. Further, 2.06±1.286 know the causes of antisocial behaviour, with an average knowledge of 41.2 percent; 3.10±1.096 understand the impact of antisocial behaviour, with an average of 62 percent; and 3.39±1.943 know about prevention, control, and management, with 42.4 percent exhibiting average knowledge in this area.
Practices Related to Antisocial Behaviour
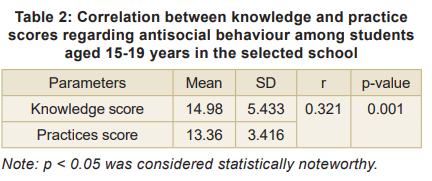
Figure 4 illustrates the distribution of practices. Overall, 85 percent of students demonstrated good practices (>50%), while 15 percent reported bad practices (≤50%). Although a slightly higher proportion maintained favourable practices, the persistence of poor practices among a considerable number of adolescents underscores the need for preventive strategies. The overall mean score for the practice level of students of the age group of 15-19 years from a selected school regarding antisocial behaviour was 13.36±3.416, and among the students, 70.3 percent had average practices regarding antisocial behaviour.
Association of knowledge and practices with demographic variables: Chi-square analysis revealed noteworthy associations between chosen demographic variables and both knowledge and practices. The knowledge scores were strongly linked (p < 0.05) with family history of antisocial behaviour (p = 0.002) and dietary pattern (p = 0.023). Similarly, practice scores Association of knowledge and practices with demographic variables: Chi-square analysis revealed noteworthy associations between chosen demographic variables and both knowledge and practices. The knowledge scores were strongly linked (p < 0.05) with family history of antisocial behaviour (p = 0.002) and dietary pattern (p = 0.023). Similarly, practice scores were strongly linked (p < 0.05) with the type of family (p = 0.027).
Correlation between Knowledge and Practices
Positive correlation exists across knowledge and practices (r = 0.321) and a noteworthy association (p < 0.05) (Table 2). Applying similar or harmonised scoring thresholds for both knowledge and practices in future studies may yield more realistic, balanced, and meaningful comparisons between these domains.
Discussion
The study focused on the ASB awareness and behaviour of adolescents aged 12 to 17 years in Imphal (Manipur). Although most adolescents reported acceptable practices, overall awareness of ASB was poor. About 60 percent showed limited understanding of its causes, effects, and prevention, likely due to the lack of systematic education and psychosocial counselling in schools (Lyngdoh et al, 2018). In contrast, 85 percent demonstrated good practices, suggesting that behaviour may be shaped by peer influence, family supervision, and social norms even in the absence of formal knowledge, a pattern also seen in other areas of adolescent health (Heap, 2020). Socio demographic factors significantly influenced outcomes: knowledge was associated with family history of ASB and dietary patterns, while practices were linked to family type, with adolescents from joint families showing better practices, possibly due to greater supervision and support (Heap, 2020; Singh et al, 2019).A moderate positive correlation between knowledge and practices (r = 0.321, p < 0.05) indicates that awareness supports better behaviour but is not sufficient on its own, underscoring the need for combined approaches involving education, counselling, peer support, and experiential learning Goldstein et al, 2017; Farrington & Loeber, 2000). The study’s strengths include its focus on adolescents in northeast India, use of a reliable structured questionnaire, and assessment of both knowledge and practices.
Limitations include purposive sampling from a single school, self-report bias, and a cross-sectional design limiting generalisability and causal inference. Future studies should use larger, multi-centric, longitudinal designs. Overall, the study stresses the need for school-based education and counselling in Northeast India, with nurses and teachers delivering evidence-based programmes to improve awareness and promote healthy behaviours that reduce adolescent antisocial behaviour. The findings support implementing structured, school-based programmes on antisocial behaviour to improve adolescents’ understanding of its causes, consequences, and prevention. Curricula should include counselling, life-skills training, and behaviour-modification activities, with parental involvement to reinforce prevention, especially for at-risk families. Future research should use larger, diverse samples and longitudinal designs to capture behavioural change over time.
From a nursing perspective, school and community health nurses play a key role in early identification, education, counselling, and prevention. Collaboration with teachers, parents, and mental health professionals, alongside involvement in policy development and age-appropriate interventions, is essential to reduce antisocial behaviour and promote psychosocial well-being.
Conclusion
The findings show that although most adolescents practice acceptable behaviours, their knowledge of the causes, consequences, and management of antisocial behaviour is limited. Noteworthy links between knowledge, practices, and demographic factors highlight the influence of family and lifestyle. The positive knowledge-practice relationship underscores the need for structured, school-based education and counselling to reduce antisocial traits and support healthy psychosocial development.
References
1. Loeber R, Farrington DP. Antisocial Behavior and Mental Health Problems: Explanatory Factors in Childhood and Adolescence. New York: Routledge; 2012
2. Loeber R, Burke JD, Pardini DA. Perspectives on oppositional defiant disorder, conduct disorder, and psychopathic features. J Child Psychol Psychiatry 2009; 50 (1-2): 133-34
3. Odgers CL, Moffitt TE, Broadbent JM, Dickson N, Hancox RJ, Harrington H, et al. Female and male antisocial trajectories: From childhood origins to adult outcomes. Dev Psychopathol 2008; 20(2): 673-716 4. Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. Psychol Rev 1993; 100(4): 674-701
5. Fergusson DM, Boden JM, Horwood LJ. Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abuse Negl 2008; 32(6): 607-19
6. Lahey BB, Waldman ID. A developmental model of the propensity to offend throughout childhood and adolescence. In: Farrington DP, ed. Integrated developmental and life- course theories of offending. New Brunswick: Transaction Publishers; 2005. pp 15-50
6. Espinoza-Romero JL, Montero-López Lena M, López-Medina E, et al. Behavioral activation system and early life parental abuse are associated with antisocial behaviours in Mexican adolescents. J Adolesc 2022; 94: 190-200
7. UN-Habitat. State of the urban youth, India 2013: Anti-social behaviour among youth at historic high. New Delhi: UN-Habitat & The Hindu; 2013
8. Ningombam S, Hutin Y, Murhekar MV. Prevalence and pattern of substance use among higher secondary school students of Imphal, Manipur, India. Int J Community Med Public Health 2022; 9(2): 837- 44
9. Lyngdoh M, Reddy CVK, Nongkynrih B, Naorem S, Zothansangi. Sleep pattern, aggressive behaviour and substance use among school students of Manipur. Indian J Public Health 2018; 62(4): 251-56
10. Heap V. Perceptions and attitudes towards antisocial behavior: Findings from a qualitative study in the UK. Crime Prev Community Saf 2020; 22(1): 1-15
11. Singh A, Gupta R, Grover S. Prevalence and correlates of aggressive behavior among school-going adolescents in India. Indian J Psychiatry 2019; 61(5): 460-66
12. Goldstein RB, Grant BF, Ruan WJ, Smith SM, Saha TD. Antisocial behavioral syndromes and four-year future psychopathology, suicidality, and functioning in the United States adult population. J Clin Psychiatry 2017; 78(1): 90-9813. Farrington DP, Loeber R. Development and risk factors of juvenile antisocial behavior and delinquency. Clin Psychol Rev 2000; 20(1): 111-36
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.