Systemic lupus erythematosus (SLE) is an autoimmune disease in which the immune system loses tolerance for self, attacking virtually every organ system and producing inflammation that waxes and wanes without warning. In the 19th century, Pierre Cazenave, a French dermatologist, used “lupus erythematosus” to describe the red, butterfly-shaped rash on the cheeks and nose, which is a hallmark of the disease. The word “erythematosus” comes from the Greek word “erythema,” meaning “redness.” This refers to the reddish rash that appears on the face of some patients with the disease. “Systemic” indicates that the disease affects multiple organ systems in the body, not just the skin. By the mid-20th century, it was recognised that lupus could involve many parts of the body, including the joints, kidneys, heart, lungs, and brain (Fanouriakis et al, 2019).
Although no cure exists, modern treatment and skilled nursing care can dramatically alter the trajectory from frequent, severe flares to long periods of stability (Whittemore & Dixon, 2008). In India, where chronic non-communicable diseases now dominate mortality and disability burden, nurses are often the healthcare professionals patients see most consistently. Helping individuals adapt physically, emotionally, and socially lies at the core of care for lupus. This article combines basic SLE knowledge with emphasis on adaptation to describe nursing methods that support patient independence and adjustment.
Methods
Design and search strategy: A narrative review methodology was employed to synthesise literature relevant to SLE and nursing adaptation. Electronic searches were conducted across major databases, including PubMed, Science Direct, and Google Scholar. Key search terms included ‘systemic lupus erythematous,’ ‘adaptation,’ ‘nursing care,’ ‘chronic illness,’ ‘self-management,’ and ‘India.’ Inclusion and exclusion criteria: Peer-reviewed articles published in English that addressed the epidemiology, pathophysiology, psychosocial impact, assessment, or nursing management of SLE were included. Both international and Indian studies were considered to ensure contextual relevance. Opinion pieces without empirical or theoretical grounding and articles with inaccessible full texts were excluded. Data synthesis: Selected articles were reviewed and thematically organised under epidemiology and aetiology, clinical manifestations, conceptual frameworks of adaptation, assessment of adaptation, and nursing interventions. Reference numbering was maintained in accordance with original sources.
Results
Epidemiology and Burden of Disease
Worldwide, roughly 5 new cases of SLE appear per 100,000 population each year, with women affected almost nine times more often than men (Tian et al, 2023). Indian figures remain uneven; community-based studies suggest an incidence of around 3.2 per 100,000, implying more than 40,000 new patients annually (The Hindu, May 2025; Malaviya et al, 1997). Yet higher rates (up to 60 per 100,000) are reported from tertiary centres, reflecting substantial under-diagnosis in rural areas (Malaviya et al, 1997). Advocacy groups such as Lupus Trust India repeatedly highlight how young women in their most productive years bear the heaviest load (Lupus Trust India, 2025). The Ayushman Bharat scheme has begun to ease financial overburden by covering costly immunosuppressants and biologics for poorer families (PM-JAY, 2025), but gaps persist.
Aetiology and Pathophysiology
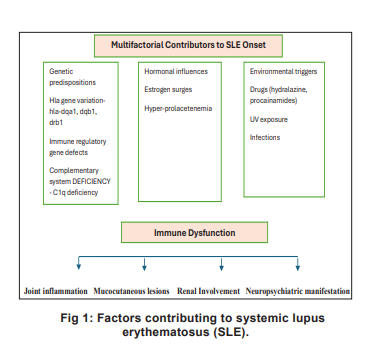
Genetic predisposition, hormonal interplay, and environmental triggers play to break immune tolerance. Over 100 risk loci have been found confirmed; defects in complement components and interferon pathways feature prominently. Oestrogen’s immunostimulatory effects help explain the striking female preponderance (Barber et al, 2021). Ultraviolet light, certain drugs, Epstein-Barr virus, smoking, and silica dust are among the best-documented triggers. Nurses can exert real influence by teaching rigorous sun protection and smoking cessation, medication adherence, infection prevention which often yields measurable reductions in flare frequency (Livneh & Antonak, 2005).
At its core, SLE involves polyclonal B-cell activation, autoantibody production, immunecomplex deposition, and complement consumption, processes that injure tissues in almost any organ (Whittemore & Dixon, 2008). Patients present with fatigue, low-grade fever, malar rash, polyarthritis, serositis, glomerulonephritis, cytopenias, or neuropsychiatric features in endlessly variable combinations (Fanouriakis et al, 2024). The capricious timing of flares is perhaps the aspect patients find most distressing.
Conceptualising Adaptation in SLE
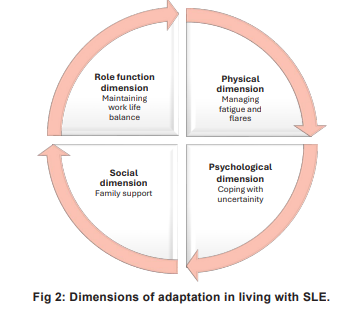
Adaptation to SLE requires continual adjustment of expectations, roles, and behaviours. The Roy Adaptation Model provides a valuable framework for understanding patient responses across four modes: physiological, self-concept, role function, and interdependence (Snyder & Lopez, 2002; Roy, 1984). Complementary perspectives include the biopsychosocial model and Lazarus and Folkman’s transactional theory of stress and coping, which emphasise appraisal, coping strategies, and available resources (Lazarus & Folkman, 1984). In the Indian context, adaptation is often complicated by cultural stigma associated with chronic illness, gender norms, financial dependency, and fragmented healthcare delivery. These factors can undermine adherence, delay care-seeking, and exacerbate psychological distress.
Assessment of Adaptation and Challenges
Effective nursing care begins with systematic assessment. Validated tools commonly used in SLE care include: the Short Form-36 Health Survey (SF-36) to assess physical and mental health status (Ware & Sherbourne, 1992); the Brief Illness Perception Questionnaire (B-IPQ) to capture cognitive and emotional representations of illness (Broadbent, 2006); and the Generalised Self-Efficacy Scale to evaluate confidence in managing challenges (Schwarzer & Jerusalem, 1995). When combined with open-ended interviews and clinical record review, these tools help uncover barriers to adaptation such as depression, fear of flares, social isolation, treatment fatigue, and low health literacy (Fanouriakis, 2024 et al; Forestier et al, 2019). Emotional reactions including denial, sadness, and anxiety, alongside practical issues such as medication non-adherence and limited access to services, are frequently identified.
Discussion
The reviewed literature underscores that adaptation to SLE is a dynamic, multifactorial process shaped by disease activity, personal coping resources, and environmental support (Fig 1). Nursing interventions that address only physical symptoms without attending to psychological and social dimensions are unlikely to achieve sustained improvement. Comprehensive, theory-guided nursing care is therefore essential. Dimensions of adaptation for those living with SLE is shown in Fig 2.
Nursing Interventions for Patients Living with SLE
Nurses play a pivotal role in bridging medical treatment prescribed by rheumatologists with daily self-management strategies that promote comfort, conserve energy, and prevent complications (Krupp, 1976). During disease flares, acute pain often manifesting as polyarthralgia with morning stiffness requires careful assessment using standardised pain scales and physical examination. Non-pharmacological measures such as heat or cold therapy, relaxation techniques, guided imagery, and gentle rangeof-motion exercises complement pharmacological management (Langham et al, 2019).
Fatigue, one of the most debilitating symptoms of SLE, necessitates systematic evaluation of contributing factors including inflammation, anaemia, depression, sleep disturbance, and medication side effects. Nurses reinforce energyconservation strategies such as pacing activities, prioritising tasks, scheduling rest periods, and using assistive devices. Optimising sleep through pain control and sleep hygiene education further supports daily functioning.
Patient education forms the cornerstone of long-term disease control. Nurses provide culturally appropriate teaching on the chronic relapsing nature of SLE, avoidance of triggers such as excessive sun exposure and infections, balanced nutrition, regular low-impact exercise, and strict adherence to prescribed medications. Emphasis is placed on the dangers of abruptly discontinuing corticosteroids and the importance of wearing medical alert identification. Early warning signs of flares and infections are reviewed repeatedly, with clear guidance on when to seek medical attention (Malaviya et al, 1997).
Medication management includes monitoring for adverse effects of antimalarials, NSAIDs, corticosteroids, and immunosuppressants, alongside infection-prevention counselling. Ongoing surveillance for complications involves regular skin and renal assessment, laboratory monitoring, and prompt reporting of new symptoms. Psychological support, including screening for anxiety and depression and referral to counselling or peer-support groups, is integral to holistic care.
Community-based resources such as teleconsultation platforms (e-Sanjeevani), structured self-management programmes, and collaboration with patient organisations enhance continuity of care and resilience (Mathias et al, 2023; Chellaiyan et al, 2019; National Digital Health Mission, 2025).
Nursing Implication
The findings of this review have important implications for nursing practice, education, administration, and research. In clinical practice, nurses should adopt an adaptation-focused, holistic approach that extends beyond symptom control to include psychosocial support, patient empowerment, and family involvement. Early identification of disease flares through vigilant assessment of subtle changes in fatigue, joint pain, rash, or mood can enable timely intervention and prevent severe complications. Nurses are well positioned to reinforce medication adherence, monitor for adverse drug reactions, and educate patients regarding trigger avoidance, infection prevention, and self-monitoring strategies.
In nursing education, greater emphasis is required on chronic illness adaptation models, autoimmune disease management, and patientcentred communication skills. Incorporating casebased learning and simulation related to SLE can strengthen clinical reasoning and preparedness among nursing students. From an administrative perspective, nurse-led clinics, structured followup protocols, and integration of telehealth services can improve continuity of care, particularly in resource-limited and rural settings.
In nursing research, further studies are needed to evaluate culturally appropriate interventions, digital health strategies, and nurseled self-management programmes that enhance long-term adaptation and quality of life among individuals with SLE.
Conclusion
Systemic lupus erythematosus remains a demanding and unpredictable illness with far-reaching implications for physical health, emotional well-being, and social participation. This review highlights that timely assessment, early recognition of flares, comprehensive patient education, and sustained psychosocial support are central to fostering adaptation. In India, where access to specialist services is uneven and the burden of chronic disease continues to rise, nurses are uniquely positioned to lead adaptationfocused care. Through theory-informed, culturally sensitive, and patient-centred interventions, nurses are uniquely positioned to lead patient education, early detection of flares, and psychosocial support. This will transform SLE from a life-limiting diagnosis into a manageable chronic condition, enabling individuals not merely to survive, but to live well.
References
1. Fanouriakis A, Kostopoulou M, Alunno A, Aringer M, Bajema I, Boletis NJ, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis 2019; 78(6): 736-45
2. Whittemore R, Dixon J. Chronic illness: The process of integration. J Clin Nurs 2008; 17(7b): 177-87
3. Tian J, Zhang D, Yao X, Huang Y, Lu Q. Global epidemiology of systemic lupus erythematosus: A comprehensive systematic review and meta-analysis. Ann Rheum Dis 2023; 82(5): 673-79
4. The Hindu. All you need to know about Lupus. 10 May 2025. https://www.thehindu.com/sci-tech/health/all-youneed-to-know-about-lupus/article69556737.ece (accessed 28 November 2025)
5. Malaviya AN, Chandrasekaran AN, Kumar A, et al. Systemic lupus erythematosus in India. Lupus 1997; 6(3): 242-46
6. Lupus Trust India. Official website. https://www.lupustrustindia.org/ (accessed 28 November 2025)
7. Pradhan Mantri Jan Arogya Yojana (PM-JAY). National Health Authority. Coverage details for chronic and autoimmune conditions including systemic lupus erythematosus under defined treatment packages. https:// pmjay.gov.in/ (accessed 28 November 2025)
8. Barber MRW, Drenkard C, Falasinnu T, et al. Global epidemiology of systemic lupus erythematosus. Nat Rev Rheumatol 2021; 17(9): 515-32
9. Livneh H, Antonak RF. Psychosocial adaptation to chronic illness and disability: A primer for counselors. J Couns Dev 2005; 83(1): 12-20
10. Snyder CR, Lopez SJ. Handbook of Positive Psychology. Oxford: Oxford University Press; 2002
11. Roy C. Introduction to Nursing: an Adaptation Model. Englewood Cliffs: Prentice-Hall; 1984
12. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer; 1984
13. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992; 30(6): 473-83
14. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res 2006; 60(6): 631-37
15. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, ed. Measures in Health Psychology. Windsor: NFER-NELSON; 1995: 35-37
16. Fanouriakis A, Kostopoulou M, Andersen J, et al. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis 2024; 83(1): 15-29
17. Forestier B, Anthoine E, Reguiai Z, Fohrer C, Blanchin M. A systematic review of dimensions evaluating patient experience in chronic illness. Health Qual Life Outcomes 2019 Jan 21; 17(1): 19. doi: 10.1186/s12955-019-1084-2
18. Krupp NE. Adaptation to chronic illness. Postgrad Med 1976; 60(5): 143-48
19. Langham J, Barut V, Samnaliev M, Langham S, Weir S, Wang X, et al. Disease severity, flares and treatment patterns in adults with systemic lupus erythematosus in the UK: A real-world observational retrospective cohort analysis. Rheumatol Advanc Pract [Internet] 2021 [cited 2025 Dec 11]; 5(3). Available from: https://dx.doi.org/10.1093/rap/ rkab061
20. Mathias EG, Dhyani VS, Krishnan JB, Rani U, Gudi N, Pattanshetty S. Community based health literacy interventions in India: A scoping review. Clin Epidemiol Glob Health 2023; 22: 101310
21. Chellaiyan VG, Nirupama AY, Taneja N. Telemedicine in India: Where do we stand? J Fam Med Prim Care 2019; 8(6):1872-76
22. National Digital Health Mission. e-Sanjeevani and related services. Ministry of Health and Family Welfare, Government of India (Accessed 28 November 2025)
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.