Monkey pox (mpox), a re-emerging zoonotic viral disease, is an emerging public health concern, particularly in low and middle-income countries. The recent global outbreaks highlighted the importance of early recognition, infection prevention, and healthcare preparedness (WHO, 2022). Studies at national and global levels have emphasised that adequate knowledge and favourable attitudes among healthcare professionals (HCPs) are essential for effective prevention and control of emerging infections (Ghazy et al, 2022; León-Figueroa et al, 2024). In India, sporadic mpox cases have been reported in 2022, 2024 and 2025 underscoring the need to assess preparedness among healthcare professionals and learners (NCDC, 2024).
Despite availability of national guidelines in India, evidence on mpox preparedness among HCPs and health profession curricula (HCPC) remains limited. Studies report variable and often suboptimal knowledge and attitudes, particularly regarding transmission, diagnosis, and prevention (Gandhi et al, 2024; Rawat et al, 2023; Sharma et al, 2023). Prior training and clinical exposure are associated with better preparedness, whereas learners often demonstrate lower awareness due to limited exposure or integration into curriculum (Belayneh et al, 2022; Ricco et al, 2023; Nguyen et al, 2023; Zhang et al, 2023). In the Indian context, limited region-specific evidence highlights the need to assess gaps in knowledge and attitudes towards mpox to inform targeted educational and training interventions.
Objectives
The primary objectives of this study were to: (1) assess the knowledge and attitude regarding mpox and its prevention among HCPs and learners; (2) compare the knowledge and attitude scores between HCPs and learners; and (3) determine the association between socio demographic variables and the knowledge as well as attitude levels of HCPs and learners. The secondary objective was to examine the relationship between knowledge and attitude scores of the HCPs and learners.
Review of Literature
A cross-sectional study in Gujarat (Gandhi et al, 2024) reported moderate knowledge and mixed attitudes towards mpox among undergraduate and postgraduate learners, highlighting the need for structured educational interventions. Similar gaps in understanding of transmission and prevention were observed among medical learners and graduates across India (Rawat et al, 2023). Suboptimal knowledge among undergraduate learners in Bihar further emphasised the importance of curriculum integration (Sharma et al, 2023). Among healthcare professionals in Kerala, awareness varied, with better knowledge linked to prior training (Mathew et al, 2023). These findings suggest that training, curriculum exposure, and clinical experience influence knowledge and attitudes towards mpox.
International studies report similar trends. Inadequate knowledge and preventive behaviours have been observed among medical and nursing learners in Vietnam, along with limited preparedness among Chinese medical learners (Nguyen et al, 2023; Zhang et al, 2023). Although healthcare professionals generally recognise the seriousness of mpox, gaps persist in infectioncontrol practices and vaccination awareness (Belayneh et al, 2022; Ghazy et al, 2022). These findings highlight the need to assess knowledge and attitudes among both healthcare professionals and learners to strengthen preparedness.
Materials and Methods
This study was a cross-sectional survey at a tertiary care centre in Bhopal (Madhya Pradesh). The sample size was calculated using the formula n = Z2 pq / d2 where Z = 1.96, p = 0.1, q = 0.9, and d =0.05. Based on this, the initial estimated sample size is 138. After accounting for a 20 percent nonresponse rate, the adjusted sample size becomes 166. As the study includes two groups (health care professionals and learners), the sample size was appropriately doubled, resulting in a total of 332 participants. Participants available during period of data collection, and willing to participate in the study were included. Convenience sampling technique was used.
A structured, researcher-developed knowledge questionnaire with 20 multiple choice items was used to assess knowledge, and a 15-item five-point Likert scale assessed attitude. The knowledge questionnaire was developed primarily based on Ministry of Health and Family Welfare Guidelines dated 14 July 2022 and included items on: global response and public health (2), causes, risk factors and transmission (5), pathophysiology and signs & symptoms (4), diagnostic evaluation (2), treatment and management (2), and prevention and control (5). Each correct response was scored as one and maximum score was 20. The statements in attitude scale were framed in terms of perceived susceptibility (2), perceived severity (1), perceived benefits (6), perceived barriers (4), perceived selfefficacy (1) and perceived threat (1). Each item was scored in the range of 1 (strongly disagree) to 5 (strongly agree). Five statements were negative, which were reverse scored.
The content validity of tools was established by sending the tool to nine experts. The internal consistency (Cronbach’s alpha) reliability of knowledge questionnaire was 0.702 and attitude scale was 0.843. The knowledge score were categorised as poor knowledge (15). Attitude score was described as favourable (>56.25), satisfactory (37.5 to 56.25) and unfavourable (<37.5).
The socio-demographic proforma had two sections: Part A for HCPs and Part B for learners. In this study, Junior Residents, Senior Residents, Nursing Officers, and Senior Nursing Officers were considered as HCPs. Learners included students of final year BSc (Hons) Nursing (already in internship) and MBBS programme (those proceeding to write the final exam before proceeding to internship).
Ethical approval from the Institutional Ethics Committee, permission from respective Deans and Medical Superintendent, and informed consent from participants were obtained. Anonymity and confidentiality of data were ensured. Data were collected in person during August–September 2025. HCPs were approached individually and provided study information, while learners were briefed in classroom settings. Consenting participants accessed and submitted the questionnaire via a QR code-linked Google Form. Measures were taken to prevent discussion or external consultation during data collection. Data were analysed using Statistical Package for Social Science (SPSS) version 20.
Results
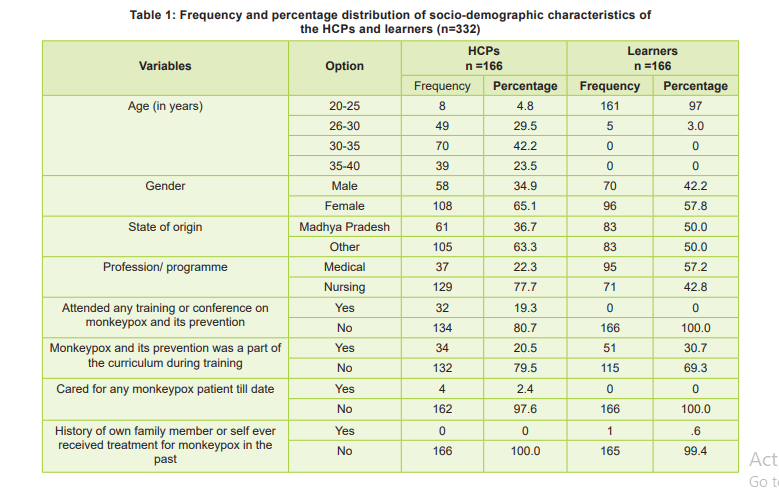
Among HCPs, 27.1 percent were senior nursing officers, 50.6 percent were nursing officers, 18.1 percent were Junior Residents, and 4.2 percent were Senior Residents (Table 1). Among resident doctors, 17.5 percent were post graduates; among nurses, 72.3 percent were graduates and 4.2 percent post-graduates. About 75.3 percent of HCPs had total clinical experience of less than five years, and only 25.9 percent had teaching experience.
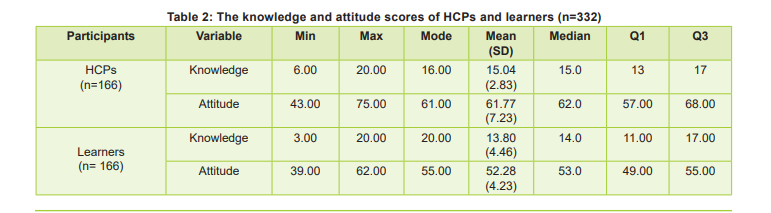
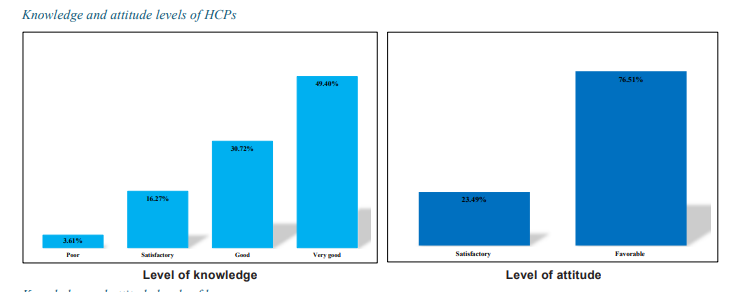
The level of knowledge and attitude of HCPs and learners is presented in Figure 1; the knowledge and attitude scores are presented in Table 2, knowledge and attitude scores being continuous and discrete variables respectively in this study. Table 2 shows that data is not normally distributed. Mann-Whitney U-test was used to compare the scores. A statistically significant difference was observed in knowledge (U=11940, p<0.035, d=0.12) and attitude (U=3717.5, p<0.001, d=0.62) score between HCPs and the learners. The effect size d shows that the observed statistically significant difference for knowledge is small and for attitude is medium to large. To identify the relationship between the knowledge and attitude scores of HCPs and the learners, Spearman’s rank correlation test was applied. The relationship between knowledge and attitude was positive, though it was moderate among HCPs (rho = 0.431, p < 0.001) and weak among the learners (rho= 0.200, p = 0.01). This implies that better knowledge can improve the attitude of health care providers.
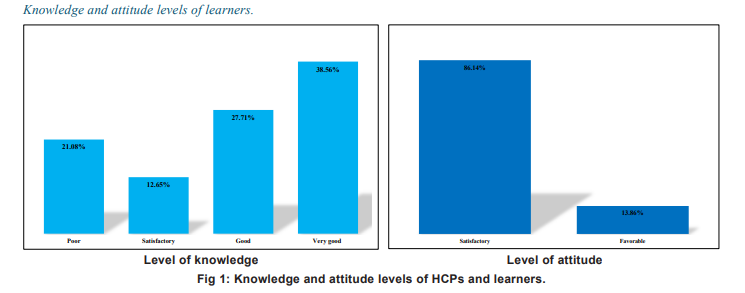
Associations between socio-demographic variables and levels of knowledge and attitude among HCPs and learners were assessed using the chi-square or Fisher’s exact test. Among HCPs, knowledge was not significantly associated with any variables (p > 0.05). However, attitude showed statistical association with age (χ² = 19.983, df = 3, p < 0.001), clinical experience (χ² = 5.192, df = 1, p = 0.023), and prior experience of caring for mpox patient (Fisher’s exact = 13.34, df = 1, p < 0.001). Among learners, knowledge was statistically associated with gender (χ² = 18.02, df = 3, p < 0.001) and programme/course (χ² = 18.45, df = 3, p < 0.001), while attitude was statistically associated with the programme/course (χ² = 5.49, df = 1, p = 0.019). Knowledge and attitude scores of learners of nursing programme and of female learners were higher compared to those of MBBS programme.
Discussion
The participants in this study were from different states and Union Territories of India, while nearly half of the learners were from Madhya Pradesh, representing a diverse participant group. The present study identified a notable gap in knowledge and attitude regarding mpox, particularly among learners. About 20 percent of HCPs reported having attended training related to mpox and its prevention or having had the topic in their curriculum. Only 30.7 percent of the learners had mpox taught in their curriculum. This finding highlights the need for strengthening training programmes or the curriculum of the healthcare programmes as an important preparedness measure to combat re-emerging infectious diseases such as mpox. Further, orientation to the existing guidelines of MoHFW regarding mpox is required at the institutional level to eventually prevent outbreak of mpox.
Higher knowledge scores and favourable attitudes were observed among HCPs in the present study. Attitude of HCPs towards mpox was associated with clinical experience. Only 2.4 percent of HCPs reported previous experience of caring for patients with mpox, as the number of diagnosed cases in India were less. Das et al (2024) reported that 71-78 percent of nurses across Bangladesh, Saudi Arabia, and Nigeria, had a positive attitude, a finding similar to the 76.5 percent of HCPs demonstrating a favourable attitude in our study where majority of the HCPs (77.6%) were nurses. The nursing curriculum in India highlights the importance of infection control and prevention from the first year of graduate or diploma nursing programmes and this could be one of the factors contributing to the higher score of attitude among nursing students.
An increase in knowledge has been consistently associated with better preventive attitudes and practices among healthcare workers (Ghazy et al, 2022; Leon-Figueroa et al, 2024). In the present study, knowledge and attitude scores showed a statistically significant positive relationship, indicating that strengthening the knowledge of learners or HCPs may improve their attitudes toward mpox and its prevention. Introduction of competency-based curriculum in MBBS and nursing programmes in India brings hope in improving the knowledge and attitude of learners; thus there is a need to monitor the change in knowledge and attitude levels irrespective of outbreak of mpox in the region.
Comparable trends in mpox knowledge have been reported with wide variation in percentages. A study from Gujarat, India, reported adequate knowledge among 78.1 percent of undergraduate and 92.1 percent of postgraduate learners (Gandhi et al, 2024). Similarly, Sharma et al (2023) reported that less than 40 percent of medical learners demonstrated good knowledge regarding mpox, indicating persistent gaps among learners across different regions of India. Our findings also suggest that the nursing programme places greater emphasis on emerging and re-emerging infectious diseases such as mpox. However, similar efforts should also be strengthened within the MBBS curriculum for preparedness and awareness regarding such public health threats.
Overall, the findings of the present study are consistent with those at national and international levels although knowledge and attitude gaps remain, especially among learners in India. Targeted educational interventions, curriculum integration, and structured training programmes are therefore essential to improve preparedness for mpox and other emerging infectious diseases.
Implications: Knowledge and clinical exposure/ experience had association with the attitude. Since learners are the future health care providers, competency-based education should consider training the learners in mpox prevention and control.
Limitation and Recommendation:The present study was limited to a single setting. Further studies may be planned to provide structured training on mpox prevention and outbreak preparedness to HCPs and learners, to assess effectiveness of such training on their knowledge and attitude.
Conclusion
HCPs demonstrated higher knowledge and more favourable attitudes towards mpox than learners and the difference was statistically significant between learners and the professionals. The observed correlation between knowledge and attitude as well as the association between attitude and clinical experience or the programme of study highlights scope to strengthen the level of awareness and knowledge on mpox and its prevention, through training programmes or by integrating the topic to the curriculum. Above all, preparedness of healthcare providers to address diseases of global concern requires due attention.
1. World Health Organization. Multi-country Monkeypox Outbreak: Situation Update. Geneva: WHO, 2022. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396
2. Ghazy RM, Ashmawy R, Taha SHN, Omran D, Hassan AA, Elhadi YAM, et al. Monkeypox knowledge and attitudes among healthcare workers: A global systematic review and meta-analysis. BMJ Open 2022; 12: e072654. Available from: https://bmjopen.bmj.com/content/12/12/e072654
3. León-Figueroa DA, Barboza JJ, Siddiq A, Sah R, Valladres MJ, Rodr MAJ, et al. Knowledge and attitudes toward mpox: A systematic review and meta-analysis. PLoS One 2024; 19(4): e0308478. Available from: https://journals.plos.org/ plosone/article?id=10.1371/journal.pone.0308478
4. National Centre for Disease Control (NCDC). CD alert on mpox (monkeypox). New Delhi: Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India, 2024 Aug. Available from: https:// ncdc.mohfw.gov.in
5. Centers for Disease Control and Prevention. Monkeypox (mpox) Outbreak Global Map. Atlanta: CDC; 2023. Available from: https://www.cdc.gov
6. Ministry of Health and Family Welfare. Guidelines for management of monkeypox disease. New Delhi: MoHFW, 2022. Available from: https://ihpoe.mohfw.gov.in/RTI/Monkeypox%20Guidelines.pdf
7. Gandhi RK, Lakum NR, Patel M, Solutia S, Kundal TS, Murugan Y. Knowledge, attitudes, and practices regarding monkeypox (mpox) among undergraduate and postgraduate learners in Gujarat, India. Cureus 2024; Sep 13, 16 (9): e85307. Available from: https://www.cureus.com/articles/85307
8. Rawat A, Jain R, Yadav P. Awareness and apprehensions regarding monkeypox among medical undergraduates and interns: A cross-sectional study from India. Cureus 2023; 15(8): e43479. Available from: https://www.cureus.com/ articles/43479
9. Sharma D, Mehta R, Singh D. Knowledge and awareness of monkeypox among undergraduate medical learners in India: A multicentric study. J Educ Health Promot 2023; 12: 94. Available from: https://www.jehp.net
10. Mathew T, Jacob J, Varghese A, Thomas B, Nair S, Joseph P, et al. Knowledge and awareness of monkeypox among healthcare professionals in Kerala: An online cross-sectional survey. J Family Med Prim Care 2023; 12(3): 1784-89. Available from: https://pubmed.ncbi.nlm.nih.gov/37654831/
11. Belayneh F, Mersha A, Tadesse F, Alemu M, Apuye T, Gebremariam A, et al. Knowledge and attitude toward monkeypox infection among healthcare professionals at Injibara General Hospital, Ethiopia. Front Public Health 2022; 10: 1123459. Available from: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1123459/full
12. Das D, Rahman N, Khalid M, Khan M, Ali S, Ahmed Z, et al. Knowledge and attitude regarding monkeypox infection among nurses in Bangladesh, Saudi Arabia and Nigeria. PLoS One 2024; 19(3): e0301223. Available from: https:// journals.plos.org/plosone/article?id=10.1371/journal. pone.0301223
13. Ricco M, Ferraro P, Camisa V, Zaniboni A, Bragazzi NL, Signorelli C, et al. Knowledge, attitudes and practices toward monkeypox in Southern Italian healthcare workers. Trop Med Infect Dis 2023; 8(3): 156. Available from: https://www. mdpi.com/2414-6366/8/3/156
14. Nguyen TP, Tran QH, Pham LN, Dang PT, Hoang LT, Nguyen HT, et al. Monkeypox: Knowledge and preventive behaviors among medical and nursing learners in Vietnam. BMC Infect Dis 2023; 23: 765. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-023- 08675-9
15. Zhang L, Huang X, Li Q, Chen S, Wang J, Liu Y, et al. Knowledge and perception toward monkeypox among Chinese medical learners: A nationwide online survey. Front Public Health 2023; 11: 1167892. Available from: https:// www.frontiersin.org/articles/10.3389/fpubh.2023.1167892/ full
16. World Health Organization. Multi-country monkeypox outbreak: situation update. Geneva: WHO; 2022. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396
17. National Centre for Disease Control (NCDC). CD alert on mpox (monkeypox). New Delhi: Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India; 2024 Aug. Available from: https:// ncdc.mohfw.gov.in
18. Centers for Disease Control and Prevention. 2023 monkeypox (mpox) outbreak global map. Atlanta: CDC; 2023. Available from: https://www.cdc.gov
19. Ministry of Health and Family Welfare. Guidelines for management of monkeypox disease. New Delhi: MoHFW; 2022. Available from: https://ihpoe.mohfw.gov.in/RTI/Monkeypox%20Guidelines.pdf
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.