Palliative care is an approach aimed at improving the quality of life and well-being of palliative care patients and their families facing life-threatening illnesses. It addresses physical symptoms along with emotional, social, and spiritual needs and provides continuous support to families throughout the course of illness. Early integration of palliative care reduces avoidable hospitalisations, improves symptom control, and enhances continuity of home-based palliative care services (WHO, 2022).
Globally, the need for palliative care is substantial and increasing due to ageing population and the growing burden of chronic and non-communicable diseases. Approximately 56.8 million people require palliative care annually, yet only about 14 percent of those in need receive palliative care (Khosla et al, 2012). Studies conducted in low- and middle-income countries report significant unmet needs related to pain management, psychosocial support, and continuity of care, highlighting the importance of community-based and home-based palliative care models.
In India, nearly six million people are estimated to require palliative care each year, but access remains limited due to inadequate policy implementation, shortage of trained professionals, and uneven service distribution. Previous Indian studies have demonstrated that home-based palliative care programmes improve symptom relief, caregiver confidence, and care continuity, particularly in resource-constrained settings. Kerala has been recognised for its community-oriented palliative care initiatives. However, literature also indicates persistent gaps in household-level coverage and utilisation, suggesting the need for structured and scalable interventions. Research evidence further indicates that nurse-led home-based palliative care plays a crucial role in addressing physical comfort, emotional support, and caregiver education. Studies have reported high acceptability of nurseled interventions, with improved communication and perceived quality of care among patients and caregivers. However, existing literature predominantly focuses on clinical and service delivery outcomes, while patient- and caregiverreported outcomes such as satisfaction remain under-explored, particularly through pilot projects conducted in community settings (Biswas et al, 2022).
Satisfaction is a key indicator of quality in palliative care, reflecting the responsiveness, acceptability, and holistic nature of services provided at home. Given the limited evidence on satisfaction outcomes in nurse-led home-based palliative care programmes at the communitybased palliative care initiatives in Kerala (Faruque M 2022, et al) there is a need for preliminary studies to assess feasibility and perceived quality of care.The present study was therefore undertaken to assess the level of satisfaction among palliative care patients and their caregivers with home-based palliative care services provided in selected wards of Thrissur.
Objectives
This study was undertaken to:
Methodology
The research was carried out as a pilot study to evaluate the feasibility and satisfaction prior to the main study.
Research approach
A quantitative research approach was adopted for this study.
Research design
A descriptive pilot study with one group post-test only design was used to assess satisfaction related to home-based palliative care services.
Setting
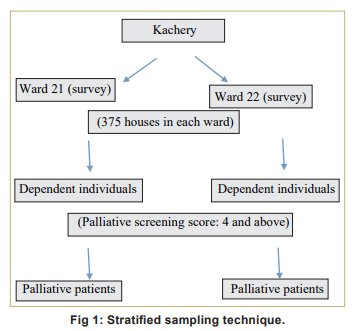
Ward No. 21 & 22 of Kachery in urban area under Thrissur Corporation. Kachery is an urban slum area under Thrissur Corporation characterised by high population density and low socio-economic conditions, making it suitable for communitybased home palliative care services. ‘Population’ here refers to patients fully dependent on palliative screening tool; the palliative care patient requires complete assistance for all activities of daily living, as assessed using the functional status domain of the Palliative Care Screening Tool.
Sample
Seven palliative patients were identified using a palliative screening tool; due to limited number of eligible patients, the study was considered a pilot. Total number of home visits and care for 7 palliative patient was 120.
Sampling technique: Stratified sampling technique (Fig 1) was adopted.
Inclusion Criteria
1. Palliative patients
2. Patients’ willingness to participate
3. Score 4 and above is indication of palliative care [Palliative screening tool adapted by Lucchetti of the centre to advanced palliative care (CPAC), Brazil 2007].
Exclusion Criteria
1. People not willing to participate
2. Scoring <4 is - no indication of palliative care [Palliative screening tool adapted by Lucchetti of the Centre to Advanced palliative care (CPAC), Brazil 2007].
Tool and Technique
Tool 1
Palliative screening tool: Lucchetti’s Centre to Advance palliative care (CPAC), Brazil 2007 the Palliative Care Screening Tool (PCST), adapted in Brazil has demonstrated high validity and reliability for identifying patients in need of palliative care, found a perfect agreement of 1.0 (Kappa test) (Lucchetti et al, 2024). It is composed of 4 domains, which include baseline disease, associated diseases, and functional status of the patient and patient personal condition. Based on the score, patients having 4 and above is taken as palliative patients (WHO, 2024).
Scoring 0-3 points: No indication of palliative care; ≥ 4 points: Indication of palliative care.
Tool 2
Part A: Socio-demographic and clinical data questionnaire: This tool assesses the sociodemographic and clinical background of the patient under 14 questions which include name, age, sex socioeconomic status, mobility, diagnosis, ability to perform ADLs etc.
Part B: Tool to assess satisfaction level on home based palliative care: It includes 12 items under 3 domains - psychosocial, physical, supportive with 4-point scale. At the end patient’s or care taker’s verbatim is collected on how much they are satisfied about the home-based palliative care.
Data Collection and Implementation of Care
After receiving palliative care training from recognised pain and palliative care agency, Thrissur and obtaining permission from authority and research committee, the survey was conducted on 7 palliative patients identified in Kachery, wards 21& 22. Following an informed consent from patients, assigned 2 students for each patient and visited those houses thrice a week and provided comprehensive care to the patient for one hour for 5 months and had visited 120 times. Wheelchair was provided in coordination with ‘Swandhanam’ palliative agency; also supplied medicine, provided basic care like wound dressing and demonstrated dressing technique for care takers for improving capacity building, BP monitoring, GRBS monitoring; provided back care, feeding, ROM exercises and counselling.
One patient passed away and we fulfilled his last wish to see the outside world by providing a wheelchair in collaboration with the palliative care society Swandhanam.
After the completion of visits and care, the level of satisfaction among the caretakers and patients was assessed using a tool based on three domainspsychological, physical, support. Verbatim of caregivers was gathered, and descriptive statistics like frequency and percentage were used to examine the data.
Results
The results of the study are shown in Tables 1 and 2.
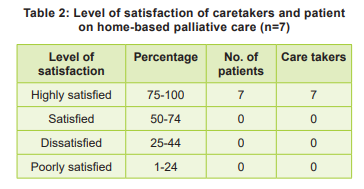
All patients and care takers in the family were satisfied with palliative care based on verbatim of caretakers under three domains- psychological, physical, support services in terms of emotional support, way of interaction and communication, feeling of comfort, quality of care, information and services, prognosis, pain relieving measures, follow-up, referrals, care received, availability of needy resources and improvements in knowledge and skill of caregivers related to dressing and other basic services.
Discussion
dentifying individuals needing palliative care using palliative screening tool (PCST)
Identified 8 dependent individuals in Kachery wards 21& 22 using survey. After screening with Palliative Care screening tool (PSCT) 7 fully dependent individuals were selected from the dependent individuals with score 4 and above; a total of 120 visits were conducted for palliative care.
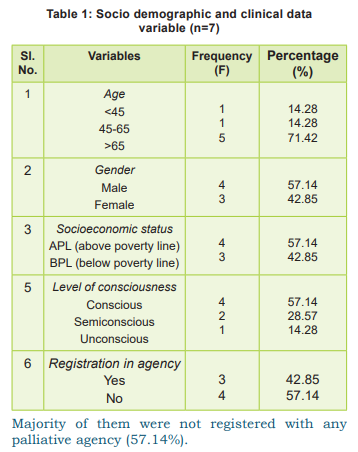
Evaluate the selected sociodemographic and clinical variables
The majority of the patients were males (57.14%) with age more than 65 years (71.42%) and most of them belong to above poverty line (57.14%). More than half the patients were partially dependent (57.14%) and full dependent (42.88%). Most of the patients were conscious (71.42%), others were semiconscious (28.57%), unconscious (14.28%). Most of them were not registered with any palliative agency (57.14%).
Assessing the satisfaction among caretakers and patients on home-based palliative
All the patients and their caretakers were fully satisfied on home-based palliative care in terms of emotional support, way of interaction and communication, feeling of comfort, quality of care, information and services, prognosis, pain relieving measures, follow-up, referrals, care received, availability of needy resources and improvements in knowledge and skill of caregivers. Verbatim of patient and caretakers was collected. They were highly satisfied about the care provided by nursing team. These findings are consistent with those of Biswas et al (2022) in Bangladesh, which reported high levels of satisfaction among cancer patients receiving home-based palliative care, especially related to emotional support, communication and pain management. Similarly, Balasubramanian et al (2022) from Kerala reported high patientsatisfaction with home-based and e-palliative care services, emphasising improved comfort, continuity of care and care givers confidence. The high satisfaction observed in the present study may be attributed to the regular home visits, individualised nursing care, effective communication and holistic approach addressing physical, psychological, and supportive needs. These results support the concept that homebased palliative care enhances quality of life and reduces the burden on patients and caregivers, particularly in community settings. Although the sample size was small, the findings align with existing literature, indicating that home-based palliative care is feasible and acceptable model of care in low- and middle-income settings such as India.
Verbatim of patient and caretakers described their satisfaction about the care provided by nursing team. The interaction of students with patients and caretakers was friendly. They mentioned about education provided by students such as cleaning and sterilisation of dressing materials in home and maintenance of aseptic techniques. They were happy that students cared patients regularly with full dedication and spirit and the quality of being thankful. The high level of satisfaction reported in this pilot study should be interpreted cautiously. Palliative care patients and caregivers may show more pleasure as a result of their appreciation for obtaining home-based services. Furthermore, regular nurse-led home visits may have had a novelty effect that significantly raised satisfaction levels.
Ethical clearance
Ethical committee approval was received from institutional ethical committee. Written consent was obtained from the participants to take part in the study. The study was internally and externally peer-reviewed.
Study limitations
The small sample size of the study, conducted as a pilot study among fully dependent palliative patient in selected wards, limits the generalisation of the findings. The small sample size and post-testonly design further limits the ability to attribute satisfaction solely to the intervention. Future studies with larger samples, comparison groups, and longer follow-up periods are recommended to minimise these biases and strengthen causal inference.
Recommendations
- A wide scale study with a larger sample size should be conducted to generalise the findings. Similar studies can be carried out in different settings, urban and rural.
- Training programmes for nurses and caregivers should be strengthened to enhance the quality of palliative care services.
- Community awareness programmes should be organised to improve utilisation of palliative care services.
The findings of this pilot study provide preliminary evidence to support the introduction of nurse. led home-based palliative care services in community setting.
Nursing Implications
Nursing practice
Community health nurses can play a crucial role in delivering home-based palliative care by providing a holistic care that addresses physical comfort, emotional support, symptom management and care giver education.
Nursing education
Nursing curricula should emphasise palliative care training, communication skills, and home-based care models to prepare students for communityoriented end of life care.
Nursing administration
Nursing administrators can utilise the findings to strengthen nurse led home-based palliative care programmes and encourage collaboration with local palliative care agencies.
Nursing Research
The pilot study highlights necessity of larger, systematic studies to generate strong evidence regarding the effectiveness of in-home palliative care services.
Conclusion
Patient satisfaction is one of the important quality indicators of health care service. Despite the limitations, overall satisfaction with the care provided by the home care team is high. The finding of this pilot study indicates that home-based palliative care is a feasible, acceptable and patientcentred approach, particularly in community settings with limited resources.
References
1. http://https://www.who.int/news-room/fact-sheets/ detail/palliative-care 5 August 2020
2. Khosla D, Patel FD, Sharma SC. Palliative care in India: Current progress and future needs. Indian J Palliat Care 2012 Sep; 18(3): 149-54 doi: 10.4103/0973-1075.105683. PMID: 23439559; PMCID: PMC3573467.
3. Biswas J, Faruque M, Banik PC, Ahmad N, Mashreky SR. Satisfaction with care provided by home-based palliative care service to the cancer patients in Dhaka City of Bangladesh: A crosssectional study. Health Sci Rep 2022 Oct 29; 5(6): e908. doi: 10.1002/hsr2.908. PMID: 36320648.
4. Balasubramanian S, Biji MS, Ranjith MK, Abina SS Patient satisfaction in home case services through e-Palliative case-An experience of terfidey cancer centre from kerala Indian J Pallative Case 2022 Jul-sept, 25 (3): 250-55.
5. Lo C, Burman D, Hales S, Swami N, Rodin G, Zimmermann C. The FAMCARE-Patient scale: measuring satisfaction with care of outpatients with advanced cancer. Eur J Cancer 2009 Dec; 45(18): 3182-88. doi: 10.1016/j.ejca.2009.09.003.
6. Lucchetti G, Neto BMA, Ramos CAS, Faria CF, Granero LA, Pires LS, et al. Use of a palliative care screening tool in elderly from a nursing home. Geriatrics Gerontology and Aging 2024; 3(3). ISSN 2447-2115, ISSN (Online) 2447-2123.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.