Universal health coverage (UHC) is a central objective of health systems globally and is included in the Sustainable Development Goals (SDGs) to ensure access to essential health services without financial hardship. In many low-and middle-income countries, including India, high out-of-pocket expenditure remains a major barrier to timely and equitable healthcare, often leading to catastrophic spending and impoverishment of households (WHO, 2021). Strengthening public financing mechanisms and expanding health insurance coverage are therefore critical strategies to achieve equity and improve population health outcomes.
In response to these challenges, the Government of India launched Ayushman Bharat in 2018 as a flagship national health reform programme aimed at transforming the healthcare delivery system. The programme comprises two major components: the establishment of Health and Wellness Centres to provide comprehensive primary healthcare and the Pradhan Mantri Jan Arogya Yojana (PMJAY), which offers cashless hospitalisation coverage of up to `5,00,000 per family per year for secondary and tertiary care to economically vulnerable populations (MoHFW, 2018). Ayushman Bharat is one of the largest publicly funded health protection schemes in the world having a pivotal role in universal health coverage. Despite wide coverage and rapid expansion, the services remain suboptimal, particularly in rural and socioeconomically disadvantaged communities. Many studies have reported limited knowledge regarding eligibility criteria, benefit packages and enrolment procedures, along with barriers such as low health literacy, procedural complexity, lack of empanelled hospitals and poor accessibility (Shrivastava et al, 2020; Gupta & Roy, 2021). These gaps between policy intent and communitylevel implementation may reduce the effectiveness of the programme and perpetuate inequities in healthcare utilisation.
Global scenario:Universal Health Coverage (UHC) has emerged as a global health priority, embedded within SDG (Shrivastava et al, 2020; Prinja et al, 2017), which aims to ensure access to quality essential health services and financial risk protection for all. According to the WHO, nearly 2 billion people worldwide face catastrophic health expenditure, and approximately 800 million people spend more than 10 percent of their household income on healthcare annually. Many countries have adopted publicly financed health insurance models to achieve UHC. In United Kingdom, National Health Service (NHS) provides tax-funded universal coverage. Thailand’s Universal Coverage Scheme (UCS) significantly reduced out-of-pocket expenditure and improved equity. In social health insurance models of Germany & Japan enrolment is mandatory. United States has mixed system including Medicare and Medicaid for vulnerable populations.
In low- and middle-income countries (LMICs), expanding financial protection remains a major challenge due to limited public health spending and high out-of-pocket expenditure. India’s Ayushma Bharat covers approximately 500 million beneficiaries. It represents a significant step towards achieving UHC in the South-East Asia. However, without adequate community awareness and simplified procedures, financial protection schemes may fail to reach intended beneficiaries.
Need for the study: The landmark Ayushman Bharat programme has expanded rapidly across India, but its benefits are not being fully realised by the intended beneficiaries, particularly in rural and underserved areas. Inadequate awareness, limited understanding of eligibility and benefit packages, and administrative barriers continue to restrict effective utilisation of the services. The planning of effective community-based interventions requires reliable data on existing levels of knowledge, utilisation patterns, and perceived barriers within the community. Although a growing body of literature is available on Ayushman Bharat, region-specific evidence from rural Uttar Pradesh, particularly Agra district, remains limited. Present study sought to assess the knowledge and utilisation of Ayushman Bharat health services among community people in Bichpuri village of Agra (UP), and to examine the association between selected socio demographic variables and utilisation patterns.
Review of Literature
Shrivastava et al (2020) reported that although most respondents had heard about the Ayushman Bharat scheme, proper knowledge regarding eligibility criteria, benefit packages and empanelled hospitals was limited. Similarly, Gupta & Roy (2021) observed that mass media and frontline health workers were the main sources of information; however, misconceptions and incomplete understanding remained common among beneficiaries.
Utilisation patterns of Ayushman Bharat services have also been explored. Kumar & Singh (2019) found that only a small proportion of eligible households had actually utilised hospitalisation benefits under PMJAY, despite being enrolled in the scheme. Low utilisation was attributed to lack of awareness, difficulty in documentation, and limited availability of nearby empanelled hospitals. Jain et al (2019) reported that rural populations were less likely to utilise cashless services compared to urban populations due to transportation barriers and poor referral mechanism.
Socio-demographic factors have also shown to have significant role. Higher educational status, better socioeconomic position and previous exposure to hospital services were associated with improved awareness and greater utilisation (Shrivastava et al, 2020; Gupta & Roy, 2021; Kumar & Singh, 2019). In contrast, illiteracy, poverty and lack of family support were identified as major determinants of poor utilisation among rural households. Procedural complexity, delay in issuance of cards, lack of guidance at hospitals, and fear of hidden costs were commonly reported obstacles (Shrivastava et al, 2020; Gupta & Roy, 2021; Kumar & Singh, 2019). In addition, limited involvement of community health workers and inadequate community-level awareness programmes were found to hinder effective implementation of the scheme.
These findings highlight persistent gaps between policy formulation and community-level utilisation. Most studies have focused on urban settings or secondary data analysis, with fewer community-based assessments.
Objectives
The study was set with following objectives:
1. To assess the level of knowledge regarding Ayushman Bharat health services;
2. To determine the extent of utilisation of Ayushman Bharat health services;
3. To identify the association of socio-demographic variables with (a) knowledge, and (b) utilisation;
4. To explore perceived barriers to utilisation.
Material and Methods
A community-based cross-sectional descriptive research design was adopted to assess the knowledge and utilisation of Ayushman Bharat health services among community people. The study was conducted in Bichpuri village of Agra district, UP, which is a predominantly rural area with a population largely dependent on public health services. The target population comprised adult men and women aged 18-65 years residing in Bichpuri village for a minimum period of one year.
Sample size and sampling technique: A sample of 300 respondents was selected using systematic random sampling technique. Households were selected at regular intervals from the village household list, and one eligible adult from each selected household was included in the study.
Inclusion and exclusion criteria: Adults aged 18-65 years who were permanent residents of the village and willing to participate in the study were included. Individuals who were seriously ill, mentally challenged, or not available at the time of data collection were excluded.
Research Tool
Data were collected using a structured interview schedule developed by the investigator. The tool consisted of four sections: Socio-demographic variables; Knowledge questionnaire related to Ayushman Bharat health services; Utilisation checklist; and Perceived barriers questionnaire.
The data collection tool was developed by the investigator after an extensive review of literature, national guidelines on Ayushman Bharat, and consultation with experts in community health nursing and public health. The tool consisted of four sections: socio-demographic variables, knowledge questionnaire, utilisation checklist, and perceived barriers scale.
Content validity: Content validity of the tool was established by a panel of experts comprising community health nursing specialists, public health experts, and medical professionals. Each item was evaluated for relevance, clarity, and simplicity. The Content Validity Index (CVI) of the tool was found to be 0.89, indicating good content validity.
Reliability of the tool: The reliability of the knowledge questionnaire was assessed using the split-half method. The obtained reliability coefficient (Karl Pearson’s correlation) was r = 0.82, which was further adjusted using the SpearmanBrown prophecy formula, indicating that the tool was reliable and suitable for data collection.
Data Collection Procedure and Analysis
After obtaining ethical clearance from the institutional ethics committee and permission from the concerned authorities, data were collected through face-to-face interviews using the structured schedule. Written informed consent was obtained from each participant prior to data collection and purpose was explained. The investigator visited selected households based on the sampling technique and interviewed one eligible participant from each household. Privacy and confidentiality were maintained throughout the process. Each interview took approximately 20-30 minutes to complete. Participants were assured that their responses would be kept confidential and used only for research purposes. Data collection was carried out over a specified period until the required sample size was achieved.
The collected data were coded and entered into a statistical software package for analysis. Descriptive statistics such as frequency, percentage, mean and standard deviation were used to summarise the data. Inferential statistics including chi-square test were applied to determine the association between sociodemographic variables and levels of knowledge and utilisation. A p value of less than 0.05 was considered statistically significant.
Description of the Tool
Data were collected using a structured interview schedule. The tool consisted of four sections:
Section I: Socio-demographic variables, which included age, gender, education, occupation, income, type of family, and other relevant background characteristics of the respondents. Section II i.e. Knowledge Questionnaire consisted of multiple-choice questions related to Ayushman Bharat health services, including eligibility criteria, benefits, coverage, and utilisation procedures. Section III i.e. Utilisation Checklist included items assessing whether the respondent had utilised Ayushman Bharat services, frequency of utilisation, and type of services availed. Section IV i.e. Perceived Barriers Scale assessed barriers to utilisation such as lack of awareness, procedural difficulties, accessibility issues, and other factors influencing service use.
Scoring Procedure
In Knowledge Questionnaire, each correct answer was awarded 1 mark, and each incorrect answer was given 0 mark. The total score was calculated by summing all correct responses. Based on the total score, knowledge was categorised as: Good knowledge, Moderate knowledge, and Poor knowledge (cut-off points were determined based on percentage distribution, e.g. >75% = good, 50- 75% = moderate, <50% = poor).
Under Utilisation Checklist, responses were recorded as Yes/No and summarised using frequency and percentage. Under Perceived Barriers, items were analysed descriptively based on frequency and percentage of responses.
Sample Size Calculation
The sample size for the present study was calculated using the standard formula for estimating proportion in a cross-sectional study:
Where: n = required sample size; Z = standard normal variate at 95% confidence level (1.96); p=estimated proportion of population having adequate knowledge/utilisation; q = 1−p; d= allowable error (precision). Substitution of values: Since no exact local estimate was available, p = 50% (0.5) was assumed for maximum sample size
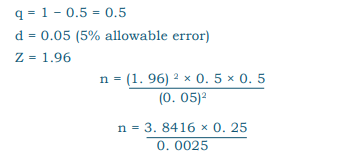
Thus, n = 384. Since the study was conducted in a limited population area (Bichpuri village) and considering feasibility, time constraints, and nonresponse, the sample size was adjusted and 300 participants were included in the study.
Sampling Technique
A systematic random sampling technique was used to select study participants.
Steps involved: (1) Preparation of Sampling Frame - a complete list of households in Bichpuri village was obtained from local records/health workers. (2) Determination of Sampling Interval (k):
(3) Selection of First Household: The first household was selected randomly using a lottery method from the first households. (4) Selection of Subsequent Households: Every kth household (e.g., every 4th household) was selected until the required sample size was achieved.
(5) Selection of Participant within Household: One eligible adult (18–65 years) was selected from each household. If more than one eligible participant was present, one was chosen using simple random (lottery) method.
Handling non-response: If a selected household had no eligible participant or refused participation, the next immediate household was included.
Results
The findings revealed that only 38 percent of respondents had good knowledge of Ayushman Bharat health services, while 32 percent had moderate knowledge and 30 percent had poor knowledge indicating that a considerable population still lacks adequate knowledge. Overall knowledge among the community can be considered moderate to inadequate. As for extent of utilisation of Ayushman Bharat health services, 27 percent of respondents had ever utilised the services, and only 18 percent had utilised them in the past year indicating low utilisation of services despite availability.
The study found a significant association between education level and knowledge. Respondents with higher education had better knowledge compared to those with lower or no formal education implying that education plays an important role in improving awareness of health schemes.
A significant association was observed between socioeconomic status and utilisation of services. Individuals with better socioeconomic conditions were more likely to utilise Ayushman Bharat services. This suggests that economic and social factors influence healthcare utilisation.
The major barriers identified were lack of awareness, procedural complexity, and distance to health facilities.
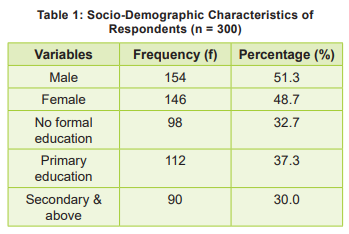
The socio-demographic characteristics of the respondents. Among the 300 participants, 51.3 percent were male and 48.7 percent female, showing a nearly equal gender distribution (Table-1). Regarding education, the majority of respondents (37.3%) had primary education, followed by 32.7 percent with no formal education and 30 percent with secondary education and above. These findings indicate that a considerable proportion of the population had low educational status, which may influence their knowledge and utilisation of Ayushman Bharat health services.
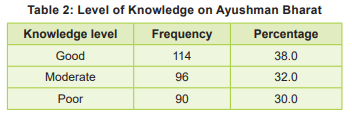
Table 2 shows the distribution of respondents according to their level of knowledge regarding Ayushman Bharat health services. Among the 300 participants, 38.0 percent demonstrated good knowledge, 32.0 percent had moderate knowledge, and 30.0 percent had poor knowledge. These findings indicate that although a proportion of respondents had adequate awareness of the scheme, a substantial segment of the population still had insufficient knowledge, highlighting the need for strengthening community-level awareness and education programmes.
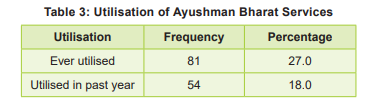
Among the participants, 27.0 percent reported that they had ever utilised Ayushman Bharat services, while only 18.0 percent had utilised the services during the past one year (Table 3). These findings reveal a low level of service utilisation in the study population, indicating possible barriers such as inadequate awareness, procedural difficulties, and limited accessibility to empanelled health facilities.
Discussion
Education level and socioeconomic status showed a significant association with both knowledge and utilisation in the present study. Respondents with higher education and better socioeconomic position demonstrated improved awareness and greater utilisation of services. These findings are in agreement with those of Jain et al (2019), who reported that literacy and economic status play a crucial role in determining health service utilisation among rural households. Low literacy and poverty may limit access to health information and reduce confidence in navigating administrative procedures, thereby restricting effective utilisation of the scheme (Shrivastava et al, 2020).
The present study also identified lack of awareness, procedural complexity and distance to health facilities as major barriers, which have been consistently reported in earlier studies and reflect persistent gaps between policy implementation and community-level utilisation (MoHFW, 2018; Shrivastava et al, 2020). The findings highlight the need for strengthening community-based awareness programmes, simplifying enrolment and claim procedures, and enhancing the role of frontline health workers in guiding beneficiaries. Improving accessibility to empanelled hospitals and strengthening referral mechanisms may further enhance utilisation and contribute to achieving the objectives of Universal Health Coverage.
Nursing Implications
Nursing practice: Community health nurses, with pivotal role in improving awareness and utilisation of Ayushman Bharat health services, should actively participate in community-based health education programmes to disseminate accurate information regarding eligibility criteria, enrolment procedures and benefit packages. They can assist beneficiaries in registration, guide them in accessing empanelled hospitals, and provide follow-up support to ensure continuity of care. Home visits and group health talks may be effectively utilised to address misconceptions and promote utilisation of services.
Nursing education: Nursing educators should incorporate updated content related to national health programmes, including Ayushman Bharat, into the nursing curriculum. Emphasis should be on developing competencies in health education, counselling and community mobilisation. Training programmes and continuing nursing education sessions should be organised to equip nursing students and staff nurses with current knowledge and practical skills facilitating enrolment and utilisation of government health schemes.
Nursing administration: Nursing administrators should strengthen supervision and coordination of community outreach activities related to Ayushman Bharat. Adequate staffing, supportive supervision and periodic in-service training can help enhance the capacity of nurses and frontline health workers. Administrators should collaborate with health authorities to organise awareness camps, enrolment drives and monitoring to improve service delivery and utilisation.
Nursing research: Nurses can undertake largescale and longitudinal studies to evaluate the impact of educational interventions and policy changes on utilisation patterns. Evidence thus generated can guide policymakers and health planners in strengthening community-based health insurance programmes and improving equitable access to healthcare services.
Recommendations
The study recommends strengthening of community-based awareness programmes to improve knowledge regarding eligibility criteria, benefit packages and utilisation procedures of Ayushman Bharat; conducting regular health education sessions and information campaigns in rural areas using simple language and audiovisual aids; promoting frontline health workers, including ASHAs, ANMs and community health nurses for active involvement in disseminating information, facilitating enrolment and guiding beneficiaries in accessing empanelled health facilities. Simplifying enrolment and claim procedures and periodic training programmes for healthcare providers are required to update them about the latest guidelines and operational aspects of Ayushman Bharat.
Conclusion
The level of knowledge and utilisation of Ayushman Bharat Health services among community people in Bichpuri village of Agra district (UP) was suboptimal. A substantial segment of the population lacked comprehensive knowledge regarding eligibility criteria, benefits and utilisation procedures. The utilisation of services was found to be low due to insufficient availability of health insurance coverage, hindering effective access to healthcare. Education level and socioeconomic status were significantly associated with both knowledge and utilisation, highlighting the influence of social determinants on health service use. Lack of awareness, procedural complexity and limited accessibility to empanelled health facilities further restricted effective utilisation of the scheme. There need for strengthening community-based awareness programmes, simplifying administrative procedures and enhancing the role of frontline health workers in facilitating enrolment and service utilisation. Focused interventions at the community level can improve equitable access to healthcare services and to achieve the objectives of universal health coverage through Ayushman Bharat.
1. World Health Organization (WHO). Tracking Universal Health Coverage: 2021 Global Monitoring Report. Geneva: World Health Organization, 2021
2. Ministry of Health and Family Welfare (MoHFW), Government of India. Ayushman Bharat – Pradhan Mantri Jan Arogya Yojana: Operational Guidelines. New Delhi: MoHFW, 2018
3. Shrivastava A, Sharma M, Kumar P. Awareness and utilisation of Ayushman Bharat scheme in rural India. J Public Health Res 2020; 9(2): 145-50
4. Gupta R, Roy A. Awareness and perception regarding Ayushman Bharat among beneficiaries in North India. Indian J Public Health 2021; 65(3): 243-48
5. Kumar R, Singh S. Determinants of health insurance utilisation in India. Indian J Community Med 2019; 44(3): 210-14
6. Jain M, Gupta S, Roy A. Barriers in utilisation of government health insurance schemes in rural populations. Indian J Community Med 2019; 44(3): 215-20
7. Prinja S, Chauhan AS, Karan A, Kaur G, Kumar R. Impact of publicly financed health insurance schemes on healthcare utilisation and financial risk protection in India: A systematic review. BMJ Open 2017; 7(6): e017099
8. La Forgia G, Nagpal S. Government-sponsored Health Insurance in India: Are You Covered? Washington, DC: World Bank; 2012
9. Garg S, Bebarta KK, Tripathi N. Performance of Ayushman Bharat–PMJAY in improving access to hospital care in India. Health Policy Plan 2022; 37(5): 625-32
10. Patel V, Parikh R, Nandraj S, et al. Assuring health coverage for all in India. Lancet 2015; 386(10011): 2422-35
11. National Sample Survey Office. Health in India: NSS 75th Round (2017-18). New Delhi: Ministry of Statistics and Programme Implementation; 2019
12. World Health Organization. Global Monitoring Report on Financial Protection in Health 2023. Geneva: WHO, 2023
13. National Health Authority. PMJAY Dashboard Report 2024. New Delhi: NHA; 2024
14. Ministry of Health and Family Welfare. National Health Accounts Estimates for India 2019-20. New Delhi: MoHFW, 2022
15. Ghosh S. Publicly financed health insurance and health service utilisation in India. Health Econ Rev 2022; 12(1): 45-53
16. International Labour Organization. Extending Social Health Protection in Asia. Geneva: ILO, 2021
17. World Bank. Universal Health Coverage Study Series: India. Washington DC: World Bank; 2022
18. Prinja S, Chauhan AS. Financial risk protection under PMJAY: Evidence from early implementation. BMJ Glob Health 2021; 6: e005519
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.