Rectus sheath haematoma (RSH) is characterised by the pooling of blood within the sheath of the rectus abdominis muscle, typically resulting from a rupture in the superior or inferior epigastric arteries or a direct tear in the muscle. While it was once thought to be uncommon, RSH is now more frequently seen in emergency rooms, largely due to the prevalent use of anticoagulant and antiplatelet medications. This condition often resembles other intra-abdominal emergencies, such as appendicitis, perforations, or ruptured aneurysms, which can lead to diagnostic errors and potentially unnecessary surgical interventions. From a nursing standpoint, RSH is particularly significant because nurses at the bedside are usually the first to notice acute abdominal pain, subtle haemodynamic changes, unexplained drops in haemoglobin, and bleeding risks associated with medication. Prompt suspicion and quick escalation of care are crucial to preventing negative outcomes.
Epidemiology and Risk Profile
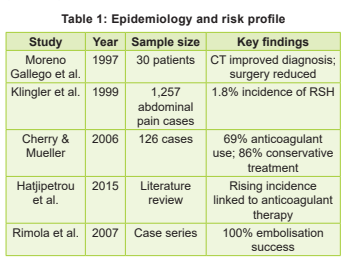
According to published studies, RSH accounts for about 1.8 percent of cases of acute abdominal pain assessed in hospitals. In a review (2006) of 126 cases at the Mayo Clinic, Cherry & Mueller (2006) found a higher incidence in older women, with nearly 70 percent of these patients using anticoagulants. More recent studies have shown a growing link with direct oral anticoagulants (DOACs). Risk factors include anticoagulation therapy, older age, chronic kidney disease, high blood pressure, severe coughing, pregnancy, abdominal trauma, and recent surgery. During the COVID-19 pandemic, therapeutic anticoagulation protocols were associated with an increase in spontaneous abdominal wall haematomas (Table 1).
Anatomy and Pathophysiology
The rectus abdominis muscles are a pair of vertically aligned muscles extending from the 5th to 7th costal cartilages to the pubis, and are separated at the midline by the linea alba. The rectus sheath, which encases these muscles, is formed by the aponeurosis of the lateral abdominal muscles. Below the arcuate line (located between the umbilicus and pubic symphysis), all aponeurotic layers pass anterior to the rectus muscle, leaving the posterior surface covered only by the transversalis fascia and peritoneum. This anatomical feature makes the lower abdomen more susceptible to haematoma formation due to reduced support from surrounding structures. The inferior epigastric artery (IEA) and superior epigastric artery (SEA) supply the muscles. The IEA, which enters the sheath at the arcuate line and runs superiorly, is particularly vulnerable because of its loose attachment and the fixed nature of its perforating branches.
During abrupt or forceful muscle contractions, shearing forces can tear the artery or its branches, particularly in the lower abdomen. The location of the rupture influences the presentation of haematoma:
- Superior epigastric artery injury typically leads to smaller haematomas that are quickly tamponaded by the complete rectus sheath.
- Inferior epigastric artery injury, especially below the arcuate line, may result in larger and more severe haematomas, as the posterior sheath is absent, allowing the haematoma to extend posteriorly, across midline, and even into the pelvic or peritoneal spaces.
To classify the severity and spread of RSH, three types are recognised:
Type I: Small, unilateral, confined within the rectus muscle.
Type II: Moderate-sized haematomas that may be unilateral or bilateral and confined within the muscle or between the muscle and transversalis fascia.
Type III: Severe, often bilateral, with extension into the peritoneum or perivesical space, and may be associated with hemodynamic instability.

showed that 83 percent of the time, CT verified the diagnosis, enabling conservative treatment for 86 percent of the patients. These results demonstrate how improvements in imaging technologies have had a direct impact on patient outcomes and treatment strategies. Similarly, in evaluation of 1,257 patients who presented with abdominal discomfort, Klingler et al (1999) found RSH in 1.8 percent of cases, indicating that the illness is under diagnosed rather than uncommon. Their research reaffirmed the value of CT and ultrasonography in distinguishing RSH from other acute abdominal conditions.
Conservative tactics are supported by recent study. In an eight-year single-centre study, Iliklerden & Kalayci (2021) found that over 90 percent of patients responded well to conservative treatment and less than 10 percent requiring surgery. This contemporary cohort analysis demonstrates that most patients can be safely managed non-operatively when early imaging and haemodynamic monitoring are used together. Liao & Puckett (2021) formalised current evidence-based practice by proposing a structured management strategy that prioritises risk assessment, early diagnosis, and the judicious use of interventional radiology. The rising prevalence of anticoagulant-associated RSH is a significant modern trend.
According to Hatjipetrou et al (2015), the rising incidence of RSH in clinical settings is probably a result of the increased usage of anticoagulant drugs. RSH, which has historically been linked to trauma, has become a common side effect of anticoagulant medication, especially in elderly persons. With a mean INR of 2.6, Cherry & Mueller (2006) found that 69 percent of patients used anticoagulants, indicating a clear correlation between anticoagulant use and the development of haematomas.
This problem has become more complicated with the introduction of direct oral anticoagulants (DOACs). DOAC-related haematomas can happen even within therapeutic dose ranges, in contrast to warfarin-associated bleeding, which frequently corresponds with higher INR levels. This demonstrates the drawbacks of determining bleeding risk exclusively using laboratory measures. Clinical monitoring is therefore crucial, especially in high-risk elderly patients.
The treatment of complex RSH situations now relies heavily on interventional radiology. According to Rimola et al (2007), percutaneous arterial embolisation produced haemostasis in every case that was treated, and most patients were released in stable condition. Comparative studies conducted recently indicate that embolisation, as opposed to surgery, lowers post-operative morbidity, hospital stay length, and transfusion needs. As a result, arterial embolisation has become a very successful technique, especially for patients who exhibit active extravasation on imaging and haemodynamic instability.
Nurses' Role
Early detection of haemodynamic instability is still mostly nurse-dependent, even with advances in technology. Before overt hypotension appears, haemodynamic deterioration in RSH may first manifest as mild symptoms such pallor, tachycardia, decreased urine production, or a declining haemoglobin level. A major contributing factor to the morbidity is the delayed detection of these warning indicators. Thus, nurse surveillance has a direct impact on the results.
From an analytical perspective, the evolution of RSH management reflects not only technological advancement but also improved interdisciplinary coordination. Modern evidence supports a graded approach.
However, the success of this algorithm is contingent on early clinical recognition, timely imaging, and vigilant bedside monitoring, in which nurses play a central role.
Emergency Management
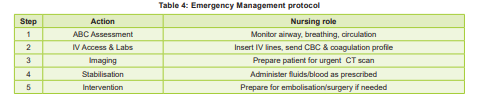
Initial nursing emergency actions include airway assessment, oxygen administration, monitoring vital signs, establishing two large-bore IV lines, and sending urgent blood investigations (Table 4).
Anticoagulants should be immediately withheld. Reversal strategies may include vitamin K, prothrombin complex concentrate, or specific antidotes, as prescribed. Intravenous crystalloids and blood transfusions were administered based on the haemodynamic status.
Haemodynamically stable patients are managed conservatively with bed rest, analgesia and monitoring. Persistent bleeding requires embolisation. Surgery is reserved for refractory cases or abdominal compartment syndromes.
Comprehensive Nursing Care
Recent literature emphasises that RSH management requires an inter professional
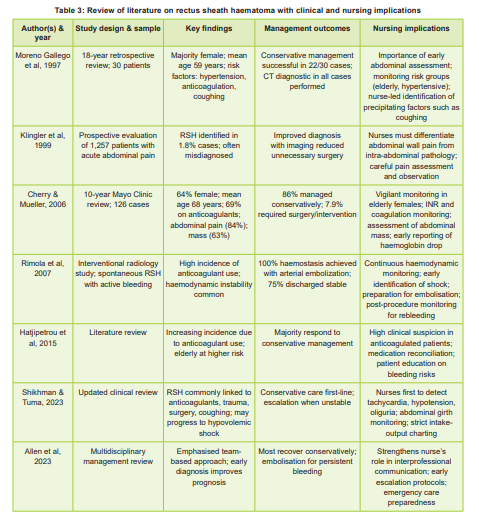
approach, with nursing care playing a central role in early recognition and monitoring. Shikhman & Tuma (2023) describe RSH as bleeding within the rectus muscle sheath, commonly associated with anticoagulant therapy, trauma, surgery, or increased intra-abdominal pressure.
Although most cases are self-limiting, elderly and anticoagulated patients are at risk of hypovolemic shock. Early symptoms such as sudden abdominal pain, localised tenderness, tachycardia, declining haemoglobin, and reduced urine output require prompt clinical suspicion. While imaging confirms diagnosis, vigilant bedside assessment—including haemodynamic monitoring, serial laboratory evaluation, and observation for haematoma progression—is largely nurse-dependent. Most stable patients are managed conservatively with rest, fluids, analgesia, and anticoagulant adjustment, highlighting the critical role of nurses in surveillance, stabilisation, and prevention of complications.
Nursing management encompasses continuous haemodynamic monitoring, pain assessment, intake and output charting, serial abdominal girth measurement, and psychological support. Education focuses on recognising early bleeding signs, adherence to medication instructions, avoiding excessive strain, and attending follow- up appointments.
Conclusion
In anticoagulant usage, rectus sheath haematoma is a significant and rising cause of acute abdominal pain. Hence, early detection and careful observation are crucial for the best results. The success of treatment is linked to quick clinical assessment and escalation of therapy. Current evidence supports a conservative-first approach for stable patients and timely embolisation for those with continuing bleeding.
Strengthening nursing competencies in anticoagulant risk assessment, emergency response protocols, and multidisciplinary communication can substantially reduce complications and prevent unnecessary surgical intervention.
Integrating structured training on acute abdominal emergencies and anticoagulantrelated bleeding into nursing education and continuing professional development is essential. The management of rectus sheath haematoma exemplifies how evidence-based nursing practice directly influences diagnostic accuracy, therapeutic decision-making, and overall patient outcomes.
1. Hatjipetrou A, Anyfantakis D, Kastanakis M. Rectus sheath hematoma: A review of the literature. Int J Surg 2015; 13: 267-71
2. Cherry WB, Mueller PS. Rectus sheath hematoma: A review of 126 cases at a single institution. Medicine (Baltimore) 2006; 85(2): 105-10
3. Klingler PJ, Wetscher GJ, Glaser K, Tschmelitsch J, Schmid T, Hinder RA. The use of ultrasound to differentiate rectus sheath hematoma from other acute abdominal disorders. Surg Endosc 1999; 13(11): 1129-34
4. Karapolat B, Tasdelen HA, Korkmaz HAA. Conservative treatment of spontaneous rectus sheath hematomas: A single center experience. Emerg Med Int 2019; 2019: 2406873
5. Carr C, Rhyne R. Diagnosis of rectus sheath hematoma by point–of-care ultrasound. J Emerg Med 2019; 56(6): 680-83
6. Smithson A, Ruiz J, Perello R, Valverde M, Ramos J, Garzo L. Diagnostic and management of spontaneous rectus sheath hematoma. Eur J Intern Med 2013; 24(6): 579-82
7. Moreno Gallego A, Aguayo JL, Flores B, Soria T, Hernández Q, Ortiz S, et al. Ultrasonography and computed tomography can reduce unnecessary surgery for abdominal rectus sheath hematomas. Br J Surg 1997; 84(9): 1295-97
8. Iliklerden UH, Kalayc? T. Treatment of rectus sheath hematomas: eight years of single-center experience with a review of literature. Ulus Travma Acil Cerrahi Derg 2021; 27(2): 222-30
9. Liao ED, Puckett Y. A proposed algorithm for the modern management of rectus sheath hematoma: A literature review. Cureus 2021;
10. (12): e20725 13. Shikhman Alexander, Tuma Faiz. Abdominal hematoma. In: StatPearls National Library of Medicine: StatPearls Publishing, 2023, Apr 10
11. Rimola Jordi, Perennedeu Joan, Falco Joan Fortuno JR, Massuet Anna, Branera Jordi. Percutaneous anterial embolization in the management of rectus sheath hematoma. AJR AM J Roentgenol 2007, June; (88(6); W 497-502. doi: 10.2214/AJR.06.0861
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.